
Rethinking Relief
DOWNLOAD THE ENTIRE SEPTEMBER 2017 NEWSLETTER including this month’s Freebie.
The United States is in the grip of an unprecedented public health crisis – and unfortunately one i n which well-meaning doctors have played a part. Due to chronic pain health issues the sales of opioid drug painkillers on prescription has quadrupled between 1999 and 2014. In 2012 alone, doctors issued 259 million opioid prescriptions – enough to give a bottle of pills to every adult in the entire United States. And in 2015 more than half of all overdose deaths in the USA involved opioids – either pain medications (such as OxyContin and Vicodin) – or illicit substances, such as opium and heroin. To put that statistic in perspective, opioids claimed roughly as many lives that year as car crashes.
n which well-meaning doctors have played a part. Due to chronic pain health issues the sales of opioid drug painkillers on prescription has quadrupled between 1999 and 2014. In 2012 alone, doctors issued 259 million opioid prescriptions – enough to give a bottle of pills to every adult in the entire United States. And in 2015 more than half of all overdose deaths in the USA involved opioids – either pain medications (such as OxyContin and Vicodin) – or illicit substances, such as opium and heroin. To put that statistic in perspective, opioids claimed roughly as many lives that year as car crashes.
Addiction is undoubtedly part of the problem, but experts now agree that the real driver behind the opioid epidemic is chronic pain. According to a landmark study published in 2011 by the Institute of Medicine, an estimated 100 million American adults live with persistent or chronic pain. Many rely on opioids just to keep moving.
There is no question that these drugs provide an excellent defence against acute, short-term pain, which alerts us to an injury or disease and subsides during recovery. But chronic pain is fundamentally different. It lingers long after an injury has healed and can produce a variety of symptoms, from headaches to body aches to crippling fatigue. It may stem from an underlying condition, such as osteoarthritis or multiple sclerosis. But it can often have no obvious source.
For some, chronic pain begins with nerve damage from diabetes, chemotherapy, a virus, a car accident or some other occurrence. In these cases, injured nerve fibres mistakenly continue to send pain signals to the brain, causing what is known as neuropathic pain.
 No matter how chronic pain starts, it often increases and spreads, leaving many people reaching or more pills. Unfortunately, higher doses of opioid drugs do not guarantee relief—and can actually make matters worse. For starters, patients build tolerance to these medications, so that over time, it takes more opioids to blunt the same levels of pain. Higher doses increase the risk of dangerous side effects, including addiction, coma and death. And recent research shows that even relatively low doses of opioids can also cause hyperalgesia, or an increased sensitivity to pain: sometimes these drugs intensify the very pain they are meant to suppress.
No matter how chronic pain starts, it often increases and spreads, leaving many people reaching or more pills. Unfortunately, higher doses of opioid drugs do not guarantee relief—and can actually make matters worse. For starters, patients build tolerance to these medications, so that over time, it takes more opioids to blunt the same levels of pain. Higher doses increase the risk of dangerous side effects, including addiction, coma and death. And recent research shows that even relatively low doses of opioids can also cause hyperalgesia, or an increased sensitivity to pain: sometimes these drugs intensify the very pain they are meant to suppress.
For these reasons, a significant number of chronic pain sufferers eventually find themselves caught in a delicate – and deadly – balancing act: they need to take more opioid medications to keep their disabling pain in check while somehow dodging the drugs’ serious and life-threatening side effects. Some succeed for decades. But those who lose their footing are flooding casualty departments and hospital beds, battling withdrawal, accidental overdose and a host of other opioid-related complications.
Last year medical authorities began to respond on several fronts. In March 2016 the Centres for Disease Control and Prevention issued stricter guidelines for prescribing opioids. Contrary to what has been common practice, it advised against treating chronic pain with these drugs unless the benefits clearly outweigh the risks. The Surgeon General (Vivek Murthy) amplified that message five months later, when he wrote directly to all the nation’s health care providers— the first time any surgeon general has done so— urging 2.3 million professionals to commit to “turn the tide on the opioid crisis.”
The message is being heard. At a handful of state-of-the-art pain centres around the United States, clinicians are exploring a range of nondrug alternatives, from psychological interventions to complementary therapies. Researchers are also working on next-generation opioid drugs, along with new nonopioid pain-killers These initiatives represent the one upside to the opioid crisis: it is forcing medical professionals to revisit how they care for people in pain.
A Different Kind of Pain
 Many experts now view chronic pain as a disease in its own right. Over time it engages and changes patterns of activity in brain areas associated not only with physical sensations but with sleep, thought and emotion. No wonder that studies show that chronic pain is associated with higher rates of mortality, sleep disorders, depression and anxiety.
Many experts now view chronic pain as a disease in its own right. Over time it engages and changes patterns of activity in brain areas associated not only with physical sensations but with sleep, thought and emotion. No wonder that studies show that chronic pain is associated with higher rates of mortality, sleep disorders, depression and anxiety.
Many chronic pain patients take a cocktail of drugs that would be deadly for a non-chronic pain sufferer. According to a Washington Post/Kaiser Family Foundation survey conducted in Autumn 2016, among people taking prescription painkillers for at least two months, about a third said they did not receive information about the dangers of opioids from their doctor. Only a third said their doctor had outlined a plan to wean them off the drugs. And another third reported that their doctor had never discussed any complementary treatments beyond medications. To treat people more effectively will require an important shift in how we think about pain – something alternative/natural medicine practitioners are well-acquainted with. Scientists are catching up in their understanding that pain is not just a sensation but a brain state and that mind-body (or body-mind) interventions may be helpful.
A team at Stanford University brings together pain psychologists, pain management physicians, psychiatrists, neurologists, anesthesiologists, physical and occupational therapists, and nurse practitioners, who collaborate to help patients safely reduce their use of opioids and replace them with non-drug alternatives. The team members meet every week to fine-tune evolving treatment plans that might incorporate cognitive-behavioural therapy (CBT), physical therapy, mindfulness training, yoga, biofeedback and acupuncture. Above all, it is a customised approach to suit the individual patient.
Turning Within
Taking such a broad approach is neither simple nor cheap – and better insurance coverage (in the USA!) of nondrug therapies will be needed to make it widely practical. Experts say the complexity of chronic pain warrants it. Perhaps the complementary therapy that has garnered the most attention in recent years is mindfulness-based stress reduction (MBSR), a clinical and more mainstream adaptation of Bu ddhist meditation practices. Jon Kabat-Zinn, now a professor of medicine emeritus at the University of Massachusetts Medical School, developed MBSR in the 1970s. Since then, MBSR classes are available in more than 30 countries. A growing body of evidence suggests that MBSR—which encourages nonjudgmental awareness of the present moment and fosters greater mind-body awareness—can mitigate a variety of ailments, from cancer and depression to drug addiction and chronic pain.
ddhist meditation practices. Jon Kabat-Zinn, now a professor of medicine emeritus at the University of Massachusetts Medical School, developed MBSR in the 1970s. Since then, MBSR classes are available in more than 30 countries. A growing body of evidence suggests that MBSR—which encourages nonjudgmental awareness of the present moment and fosters greater mind-body awareness—can mitigate a variety of ailments, from cancer and depression to drug addiction and chronic pain.
In 2016 Daniel Cherkin and his colleagues tested three treatments for chronic low back pain in 342 young and middle-aged adults: MBSR, cognitive-behavioural therapy – designed to change pain-related thoughts and behaviours – and standard pain care. They found that compared with participants who received standard pain care, more patients receiving MBSR or CBT showed a significant drop in “pain bothersomeness” after 26 weeks. In addition, the MBSR and CBT groups improved more in their functional abilities.
Other chronic pain sufferers are making gains with biofeedback. Using sensors to monitor bodily signals such as muscle tension and heart rate, they build awareness of physiological processes and learn to modulate their own pain. A 2017 meta-analysis evaluated biofeedback for chronic back pain in 1,062 patients and found that it not only lowered pain intensity but also improved patients’ coping abilities and reduced the incidence of pain-related depression. Others have tested a more sophisticated technique called neuro- feedback, which provides patients with images of their own brain activity using electroencephalography or functional MRI. This kind of training can teach patients to control brain regions associated with pain processing.
Additional evidence suggests that acupuncture might help ease chronic pain in some cases. The practice remains controversial, in part because it is difficult to study. But a 2014 analysis of 29 clinical trials of acupuncture for chronic pain in nearly 18,000 patients showed that compared with treatment with no needles or misplaced needles, the traditional form – with needles placed according to centuries-old Chinese practice – produced greater pain relief. At the same time, a significant number of people in the control groups also saw benefits, suggesting a strong placebo effect.
 That finding reinforces the idea that when it comes to pain, simply being under the care of a receptive health care professional can be palliative. Researchers are investigating how all these complementary treatments work. Thankfully they don’t seem to be waiting for basic science to tell them the optimal way to treat pain. There is broad agreement that mindfulness, yoga, biofeedback and acupuncture may succeed by changing patients’ relationship to their pain rather than actually lowering the intensity of the physical sensation. If patients are suffering then it would seem logical (and human) to find what really works from the various diverging modalities available.
That finding reinforces the idea that when it comes to pain, simply being under the care of a receptive health care professional can be palliative. Researchers are investigating how all these complementary treatments work. Thankfully they don’t seem to be waiting for basic science to tell them the optimal way to treat pain. There is broad agreement that mindfulness, yoga, biofeedback and acupuncture may succeed by changing patients’ relationship to their pain rather than actually lowering the intensity of the physical sensation. If patients are suffering then it would seem logical (and human) to find what really works from the various diverging modalities available.
The NCCIH (National Center for Complementary and Integrative Health) recently conducted an extensive review of published clinical trials for a variety of complementary therapies with the aim of finding out which treatments might work best for which patients. It found that acupuncture and yoga benefited people with chronic back pain the most. Acupuncture and tai chi proved most helpful for those with chronic pain resulting from osteoarthritis. Massage therapy provided short-term benefits for neck pain, and relaxation techniques were most effective in those with severe headaches and migraines.
Feeling Your Pain
There is another reason why individualised care makes sense for chronic pain: different people can experience the same kind of pain in very different ways. In particular, researchers are discovering that how much chronic pain affects any one person depends heavily on so-called biopsychosocial factors – how someone reacts to pain emotionally, what other sources of stress exist, how much social support surrounds the person. Targeting these influences can not only reduce patients’ experience of pain but dramatically improve their quality of life. Indeed, chronic pain–related disabilities often leave people isolated and cut off from friends, which can, in turn, make the pain more intense.
To identify biopsychosocial factors up front, patients at the Stanford clinic fill out an extensive online questionnaire, capturing everything from work histories and adverse childhood experiences to sleep habits and anger levels. The practitioners there believe that collecting this type of data holds the key to matching patients with effective treatments. The questionnaire is part of a free, open-source repository that has been created, together with researchers at the NIH (National Institute of Health). The system, called the Collaborative Health Outcomes Information Registry (CHOIR), is now in use at medical centres around the USA and soon will be in several other countries. It contains data from more than 15,000 patients. Health care providers can use the system to track patients’ progress over time and to compare their trajectories with similar cases.
This data set has revealed that one factor in particular – a mindset called catastrophising – predicts the impact of chronic pain on a person’s life far better than any other measure. At its core, catastrophising is a tendency to exaggerate or magnify the threat of pain, to fear the worst and remain focused on the experience of pain. For people trapped in this way of thinking, their pain feels overwhelming. They hold little hope that they will ever be well again. That leads to a very strong desire to escape the pain, and they reach for the pain medication. Because catastrophising is such a powerful force on the experience of pain, it seems like a stroke of genius to target it.
For many this sense of powerlessness is common – and doctors who dismiss chronic pain because they cannot explain it only compound that feeling. When surgeries or other treatments fail to help, patients learn to expect failure. They become very demoralised. When patients go to the Stanford clinic the practitioners’ first job is to ‘remoralise’ them! The initial step is giving patients back a sense of control, no matter how small. They often need to know that their pain is real, that it is not their ‘fault’ and that there are some ways that it can be addressed. The patients are invited to learn about how pain and biopsychosocial factors interact. They may receive a relaxation CD so that the auditory experience recorded on the CD works to calm the nervous system. And they are encouraged to think of listening to the CD as taking a dose of mind-body medicine!
REFERENCES
■ Acupuncture for Chronic Pain. Andrew J. Vickers and Klaus Linde in JAMA, Vol. 311, No. 9, pages 955–956; March 5, 2014.
■ The Effectiveness and Risks of Long-Term Opioid Therapy for Chronic Pain:
A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop. Roger Chou in Annals of Internal Medicine, Vol. 4, No. 162, pages 276– 286; February 17, 2015.
■ National Pain Strategy: A Comprehensive Population Health-Level Strategy for Pain. Interagency Pain Research Coordinating Committee. u.S. Department of Health and Human Services, 2016. https://iprcc.nih.gov/National_Pain_Strategy/ NPS_Main.htm
■ Doctors are Breaking Away. Stephani Sutherland in Scientific American Mind, Vol. 28, No. 3, May/June 2017, pages 28-35.
■ Effect of Mindfulness-Based Stress Reduction vs Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults with Chronic Low Back Pain: A Randomized Clinical Trial. Daniel C. Cherkin et al. in JAMA, Vol. 315, No. 12, pages 1203–1299; March 22, 2016.
■ Evidence-Based Evaluation of Complementary Health Approaches for Pain Management in the United States. Richard L. Nahin et al. in Mayo Clinic Proceedings, Vol. 91, No. 9, pages 1292–1306; September 2016.
■ Efficacy of Biofeedback in Chronic Back Pain: A Meta-analysis. Robert Sielski et al. in International Journal of Behavioral Medicine, Vol. 24, No. 1, pages 25–41; February 2017.
 Evolutionary neuropsychologist Jaak Panksepp has shown that the brains of all animals contain the neural circuitry engaged in human laughter. These areas include emotional and memory centres, such as the amygdala and hippocampus. Laughter seems to bubble up from below the surface of the cortex as an involuntary response while activating the pleasure systems in the brain. Famously, Panksepp has even documented (by using technologies that allow humans to hear very high frequencies) that rats emit a rhythmic chirping sound when “tickled.”
Evolutionary neuropsychologist Jaak Panksepp has shown that the brains of all animals contain the neural circuitry engaged in human laughter. These areas include emotional and memory centres, such as the amygdala and hippocampus. Laughter seems to bubble up from below the surface of the cortex as an involuntary response while activating the pleasure systems in the brain. Famously, Panksepp has even documented (by using technologies that allow humans to hear very high frequencies) that rats emit a rhythmic chirping sound when “tickled.” Stand-up comedians often exploit expectations to make audiences laugh. They build suspense and push the boundaries of norms and acceptability to provoke our laughter, whether with puns, jokes or witty retorts. For something to be funny, the person telling a joke and the person hearing it need some common knowledge. Humour therefore requires at least some rudimentary understanding of the physical and social world. This understanding can be based on experience and observation, which provide the foundation for what is “ordinary.” With that baseline, we can differentiate the ordinary from the absurd.
Stand-up comedians often exploit expectations to make audiences laugh. They build suspense and push the boundaries of norms and acceptability to provoke our laughter, whether with puns, jokes or witty retorts. For something to be funny, the person telling a joke and the person hearing it need some common knowledge. Humour therefore requires at least some rudimentary understanding of the physical and social world. This understanding can be based on experience and observation, which provide the foundation for what is “ordinary.” With that baseline, we can differentiate the ordinary from the absurd. Most important, infants create these novel interactions. They decide when and with whom to employ these techniques. As such, these types of playful, teasing exchanges can give us a window into infants’ awareness. Teasing in particular requires at least a rudimentary understanding of others’ minds, a desire to engage, and a guess or prediction as to how to provoke the mind of someone else. To trick someone else means to know that someone else can, in fact, be tricked. This knowledge, referred to as a theory of mind, is a mature insight that has traditionally been credited only to children who are at least four years old. Although infants do not have the mind theory sophistication of older children, their ability to effectively tease and provoke others suggests they have at least some level of awareness.
Most important, infants create these novel interactions. They decide when and with whom to employ these techniques. As such, these types of playful, teasing exchanges can give us a window into infants’ awareness. Teasing in particular requires at least a rudimentary understanding of others’ minds, a desire to engage, and a guess or prediction as to how to provoke the mind of someone else. To trick someone else means to know that someone else can, in fact, be tricked. This knowledge, referred to as a theory of mind, is a mature insight that has traditionally been credited only to children who are at least four years old. Although infants do not have the mind theory sophistication of older children, their ability to effectively tease and provoke others suggests they have at least some level of awareness.
 In a pair of 2012 studies led by social psychologist Ashley Batts Allen, researchers investigating self-compassion in older adults found both psychological and practical benefits. In the first study, with 132 participants ranging from 67 to 90 years old, they found that people who were strongly self-compassionate reported a greater sense of well-being even when they were in poor health. In the second study, involving 71 seniors, self-compassion predicted how likely they were to be willing to use a walker if necessary. The self- compassionate people were just less bothered by the fact that they needed help. If you are low in self-compassion, you’re using too much emotional energy thinking about the bad feelings and not enough addressing the real issues. For example, denying one problem—insisting on not using a walker—can create further difficulties, such as a hip fracture. The mindfulness component of high self-compassion, in contrast, leads people to acknowledge and accept reality, without an emotional judgment. The common-humanity component helps, too, by, for example, allowing one to recognise that everyone has physical limitations with age.
In a pair of 2012 studies led by social psychologist Ashley Batts Allen, researchers investigating self-compassion in older adults found both psychological and practical benefits. In the first study, with 132 participants ranging from 67 to 90 years old, they found that people who were strongly self-compassionate reported a greater sense of well-being even when they were in poor health. In the second study, involving 71 seniors, self-compassion predicted how likely they were to be willing to use a walker if necessary. The self- compassionate people were just less bothered by the fact that they needed help. If you are low in self-compassion, you’re using too much emotional energy thinking about the bad feelings and not enough addressing the real issues. For example, denying one problem—insisting on not using a walker—can create further difficulties, such as a hip fracture. The mindfulness component of high self-compassion, in contrast, leads people to acknowledge and accept reality, without an emotional judgment. The common-humanity component helps, too, by, for example, allowing one to recognise that everyone has physical limitations with age. But if people find it easier to show compassion to others than to themselves, how can we understand the results from the couples study? Neff believes that being kinder to others than to yourself, though possible, will not carry people through long-term relationships.
But if people find it easier to show compassion to others than to themselves, how can we understand the results from the couples study? Neff believes that being kinder to others than to yourself, though possible, will not carry people through long-term relationships. If being self-compassionate has so many positive outcomes, can people learn to treat themselves more kindly?
If being self-compassionate has so many positive outcomes, can people learn to treat themselves more kindly? Furthermore, many people dropped out of the intervention, some actually describing intense, troubling emotions—crying uncontrollably or realising they had no uncomplicated relationships in their lives. Germer and Neff brace their workshop participants for this possibility, using the firefighting metaphor of “back draft” to explain the phenomenon: just as flames rush out of a room as oxygen returns, old pain can surface amid an influx of compassion in people starved of love. It is possible that before taking a course, some individuals may need to ease into self-compassion practice slowly, perhaps with the aid of a therapist.
Furthermore, many people dropped out of the intervention, some actually describing intense, troubling emotions—crying uncontrollably or realising they had no uncomplicated relationships in their lives. Germer and Neff brace their workshop participants for this possibility, using the firefighting metaphor of “back draft” to explain the phenomenon: just as flames rush out of a room as oxygen returns, old pain can surface amid an influx of compassion in people starved of love. It is possible that before taking a course, some individuals may need to ease into self-compassion practice slowly, perhaps with the aid of a therapist.
 A few years later a friend told Carolyn about a depression-prevention study at the University of Pittsburgh. She signed up immediately. All 247 participants were, like her, older adults with mild depressive symptoms— people who without treatment face a 20 to 25 percent chance of succumbing to major depression. Half received about five hours of problem-solving therapy, a cognitive-behavioral approach designed to help patients cope with stressful life experiences. The rest, including Carolyn, received dietary counseling. Guided by a social worker, she discovered that she liked salmon, tuna and a number of other “brain-healthy” foods—which quickly replaced all the criaps, cake and sweets she was eating.
A few years later a friend told Carolyn about a depression-prevention study at the University of Pittsburgh. She signed up immediately. All 247 participants were, like her, older adults with mild depressive symptoms— people who without treatment face a 20 to 25 percent chance of succumbing to major depression. Half received about five hours of problem-solving therapy, a cognitive-behavioral approach designed to help patients cope with stressful life experiences. The rest, including Carolyn, received dietary counseling. Guided by a social worker, she discovered that she liked salmon, tuna and a number of other “brain-healthy” foods—which quickly replaced all the criaps, cake and sweets she was eating. Sanchez-Villegas later confirmed the association in another large trial. The PREDIMED (Prevention with Mediterranean Diet) study—a multicentre research project evaluating nearly 7,500 men and women across Spain—initially looked at whether a Mediterranean diet, supplemented with extra nuts, protects against cardiovascular disease. It does. But in 2013 Sánchez-Villegas and other investigators also analysed depression data among PREDIMED’s participants. Again, compared with subjects who ate a generic low-fat diet, those who adhered to the nut-enriched Mediterranean diet had a lower risk for depression. This was especially true among people with diabetes, who saw a 40 percent drop in risk. Perhaps these patients, who cannot adequately process glucose, benefited the most because the Mediterranean diet minimised their sugar intake.
Sanchez-Villegas later confirmed the association in another large trial. The PREDIMED (Prevention with Mediterranean Diet) study—a multicentre research project evaluating nearly 7,500 men and women across Spain—initially looked at whether a Mediterranean diet, supplemented with extra nuts, protects against cardiovascular disease. It does. But in 2013 Sánchez-Villegas and other investigators also analysed depression data among PREDIMED’s participants. Again, compared with subjects who ate a generic low-fat diet, those who adhered to the nut-enriched Mediterranean diet had a lower risk for depression. This was especially true among people with diabetes, who saw a 40 percent drop in risk. Perhaps these patients, who cannot adequately process glucose, benefited the most because the Mediterranean diet minimised their sugar intake. Two meta-analyses from 2010 and 2012 collectively reviewed data from 53 studies and reported significantly elevated levels of several blood markers of inflammation in depressed patients. And numerous studies have reported increased or altered activity of immune cells called microglia—which play a key role in the brain’s inflammatory response—in patients with psychiatric disorders, including depression and schizophrenia. It is not clear whether inflammation causes mental illness in some cases, or vice versa. But the evidence suggests that many if not most known risk factors for psychiatric disorders, especially depression, promote inflammation; these include abuse, stress, grief and certain genetic predilections.
Two meta-analyses from 2010 and 2012 collectively reviewed data from 53 studies and reported significantly elevated levels of several blood markers of inflammation in depressed patients. And numerous studies have reported increased or altered activity of immune cells called microglia—which play a key role in the brain’s inflammatory response—in patients with psychiatric disorders, including depression and schizophrenia. It is not clear whether inflammation causes mental illness in some cases, or vice versa. But the evidence suggests that many if not most known risk factors for psychiatric disorders, especially depression, promote inflammation; these include abuse, stress, grief and certain genetic predilections. Our evolutionary backstory could explain these neuro-protective effects. Sometime between 195,000 and 125,000 years ago, humans may have nearly gone extinct. A glacial period had set in that probably left much of the earth icy and barren for 70,000 years. The population of our hominin ancestors plummeted to possibly only a few hundred in number, and most experts agree that everyone alive today is descended from this group. Exactly how they—or early modern humans, for that matter—managed to stay alive during recurring glacial periods is less clear. But as terrestrial resources dried up, foraging for marine life in reliable shellfish beds surrounding Africa most likely became essential for survival. Graduate student Jan De Vynck of Nelson Mandela Metropolitan University in South Africa has shown that one person working those shellfish beds can harvest a staggering 4,500 calories an hour.
Our evolutionary backstory could explain these neuro-protective effects. Sometime between 195,000 and 125,000 years ago, humans may have nearly gone extinct. A glacial period had set in that probably left much of the earth icy and barren for 70,000 years. The population of our hominin ancestors plummeted to possibly only a few hundred in number, and most experts agree that everyone alive today is descended from this group. Exactly how they—or early modern humans, for that matter—managed to stay alive during recurring glacial periods is less clear. But as terrestrial resources dried up, foraging for marine life in reliable shellfish beds surrounding Africa most likely became essential for survival. Graduate student Jan De Vynck of Nelson Mandela Metropolitan University in South Africa has shown that one person working those shellfish beds can harvest a staggering 4,500 calories an hour. In 1972 psychiatrist Michael Crawford, now at Imperial College London, co-published a paper concluding that the brain is dependent on DHA and that DHA sourced from the sea was critical to mammalian brain evolution, especially human brain evolution. For more than 40 years he has argued that the rising rates of brain disorders are a result of post–World War II dietary changes—especially a move toward land-sourced food and, subsequently, the embrace of low-fat diets. He feels that omega-3s from seafood were critical to the human species’ rapid neural march toward higher cognition.
In 1972 psychiatrist Michael Crawford, now at Imperial College London, co-published a paper concluding that the brain is dependent on DHA and that DHA sourced from the sea was critical to mammalian brain evolution, especially human brain evolution. For more than 40 years he has argued that the rising rates of brain disorders are a result of post–World War II dietary changes—especially a move toward land-sourced food and, subsequently, the embrace of low-fat diets. He feels that omega-3s from seafood were critical to the human species’ rapid neural march toward higher cognition. In one striking (if slightly nauseating) experiment in 2014, then 23-year-old student Tom Spector wiped out about a third of the bacterial species in his gut by limiting his diet to McDonald’s fast food. It took only 10 days. Spector played the guinea pig for two reasons: as a project to complete his genetics degree and to provide data for his father, Tim, a genetic epidemiology professor at King’s College London, who studies how processed diets affect gastrointestinal bacteria. The Spector family’s research did not assess specific health consequences—they were measuring only the drop in floral diversity in Tom’s gut—but Tom did report feeling lethargic and down after days of burgers, fries and sugary soda. The decline in species was so drastic that Tim sent the results to three laboratories for confirmation.
In one striking (if slightly nauseating) experiment in 2014, then 23-year-old student Tom Spector wiped out about a third of the bacterial species in his gut by limiting his diet to McDonald’s fast food. It took only 10 days. Spector played the guinea pig for two reasons: as a project to complete his genetics degree and to provide data for his father, Tim, a genetic epidemiology professor at King’s College London, who studies how processed diets affect gastrointestinal bacteria. The Spector family’s research did not assess specific health consequences—they were measuring only the drop in floral diversity in Tom’s gut—but Tom did report feeling lethargic and down after days of burgers, fries and sugary soda. The decline in species was so drastic that Tim sent the results to three laboratories for confirmation. The good news is that dietary changes can not only wreck our microbial diversity, they can boost it, reducing gastrointestinal inflammation in the process. In 2015 a group at the University of Pittsburgh conducted a study in which 20 African-Americans from Pennsylvania swapped diets with 20 rural black South Africans. In place of their usual low-animal-fat, high-fibre diet, the Africans consumed burgers, fries, hash browns, and the like. The Americans eschewed their normal fatty foods and refined carbohydrates for beans, vegetables and fish. After just two weeks the Americans’ colons were less inflamed, and fecal samples showed a 250 percent spike in butyrate-producing bacterial species. Butyrate is thought to reduce the risk of cancer. The South Africans, on the other hand, underwent microbial changes associated with increased cancer risk.
The good news is that dietary changes can not only wreck our microbial diversity, they can boost it, reducing gastrointestinal inflammation in the process. In 2015 a group at the University of Pittsburgh conducted a study in which 20 African-Americans from Pennsylvania swapped diets with 20 rural black South Africans. In place of their usual low-animal-fat, high-fibre diet, the Africans consumed burgers, fries, hash browns, and the like. The Americans eschewed their normal fatty foods and refined carbohydrates for beans, vegetables and fish. After just two weeks the Americans’ colons were less inflamed, and fecal samples showed a 250 percent spike in butyrate-producing bacterial species. Butyrate is thought to reduce the risk of cancer. The South Africans, on the other hand, underwent microbial changes associated with increased cancer risk.

 His colleague at the University of Michigan, Terry Robinson, had been using a neurotoxin to destroy dopamine neurons and create rats that modelled severe symptoms of Parkinson’s. Berridge decided to give sweet foods to these rodents and see if they appeared pleased. He expected that their lack of dopamine would deny them this response. Because they were so dopamine-depleted, Robinson’s rats rarely moved if left alone. They did not seek food and had to be fed artificially. Unexpectedly, however, their facial reactions were completely normal—they continued to lick their lips in response to something sweet and grimace at a bitter meal.
His colleague at the University of Michigan, Terry Robinson, had been using a neurotoxin to destroy dopamine neurons and create rats that modelled severe symptoms of Parkinson’s. Berridge decided to give sweet foods to these rodents and see if they appeared pleased. He expected that their lack of dopamine would deny them this response. Because they were so dopamine-depleted, Robinson’s rats rarely moved if left alone. They did not seek food and had to be fed artificially. Unexpectedly, however, their facial reactions were completely normal—they continued to lick their lips in response to something sweet and grimace at a bitter meal. This dissociation fit with studies of Parkinson’s patients. They are still, after all, able to enjoy life’s ups but often have problems with motivation. Perhaps the most vivid example of this occurred in the early 20th century, when an epidemic of encephalitis lethargica left thousands of people with an especially severe parkinsonian condition. Their brains were so depleted of dopamine that they were unable to initiate movement and were essentially “frozen in place” like living statues. (The film Awakenings, which starred Robin Williams as neurologist Oliver Sacks, was based on the doctor’s 1973 memoir of treating such patients.) But a sufficiently strong external stimulus could spark action for people with this condition. In one case cited by Sacks, a man who typically sat motionless in his wheelchair on the beach saw someone drowning. He jumped up, rescued the swimmer and then returned to his prior rigidly fixed position. One of Sacks’s own patients would sit silent and still unless thrown several oranges, which she would then catch and juggle.
This dissociation fit with studies of Parkinson’s patients. They are still, after all, able to enjoy life’s ups but often have problems with motivation. Perhaps the most vivid example of this occurred in the early 20th century, when an epidemic of encephalitis lethargica left thousands of people with an especially severe parkinsonian condition. Their brains were so depleted of dopamine that they were unable to initiate movement and were essentially “frozen in place” like living statues. (The film Awakenings, which starred Robin Williams as neurologist Oliver Sacks, was based on the doctor’s 1973 memoir of treating such patients.) But a sufficiently strong external stimulus could spark action for people with this condition. In one case cited by Sacks, a man who typically sat motionless in his wheelchair on the beach saw someone drowning. He jumped up, rescued the swimmer and then returned to his prior rigidly fixed position. One of Sacks’s own patients would sit silent and still unless thrown several oranges, which she would then catch and juggle.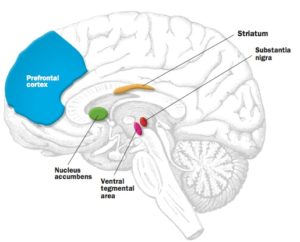
 leading causes of disability and death around the globe, according to the World Health Organisation. At any given time, it afflicts around 350 million people worldwide. Only a fraction of sufferers seek help, and of those, only a third respond to standard treatment, which is usually counselling and medication. Antidepressant drugs are often costly and can have serious side effects, driving many patients to search for less expensive, safer, more natural solutions. In a survey of more than 2,000 U.S. adults published in 2001, more than half of the respondents with depression said that they had turned to some kind of alternative treatment, such as yoga, herbal medicines or acupuncture.
leading causes of disability and death around the globe, according to the World Health Organisation. At any given time, it afflicts around 350 million people worldwide. Only a fraction of sufferers seek help, and of those, only a third respond to standard treatment, which is usually counselling and medication. Antidepressant drugs are often costly and can have serious side effects, driving many patients to search for less expensive, safer, more natural solutions. In a survey of more than 2,000 U.S. adults published in 2001, more than half of the respondents with depression said that they had turned to some kind of alternative treatment, such as yoga, herbal medicines or acupuncture. Some researchers have attempted to figure out what types of exercise and intensity levels are most effective as an anti-depressant. In a frequently cited study from 2005, for example, psychiatrist Madhukar Trivedi (University of Texas Southwestern Medical Center) and his colleagues tracked the health of 80 adults with mild to moderate depression for three months as they exercised three to five times a week on a treadmill or stationary bicycle at low intensity (seven kilocalories per kilogram per week) or at a higher intensity, as recommended by public health authorities (17.5 kilocalories per kilogram per week). At the end of the three months, the adults who exercised at the higher intensity had lessened the severity of their depression by 47 percent, compared with only 30 percent for the low-intensity group and 29 percent for a group who engaged in stretching rather than aerobic exercise.
Some researchers have attempted to figure out what types of exercise and intensity levels are most effective as an anti-depressant. In a frequently cited study from 2005, for example, psychiatrist Madhukar Trivedi (University of Texas Southwestern Medical Center) and his colleagues tracked the health of 80 adults with mild to moderate depression for three months as they exercised three to five times a week on a treadmill or stationary bicycle at low intensity (seven kilocalories per kilogram per week) or at a higher intensity, as recommended by public health authorities (17.5 kilocalories per kilogram per week). At the end of the three months, the adults who exercised at the higher intensity had lessened the severity of their depression by 47 percent, compared with only 30 percent for the low-intensity group and 29 percent for a group who engaged in stretching rather than aerobic exercise.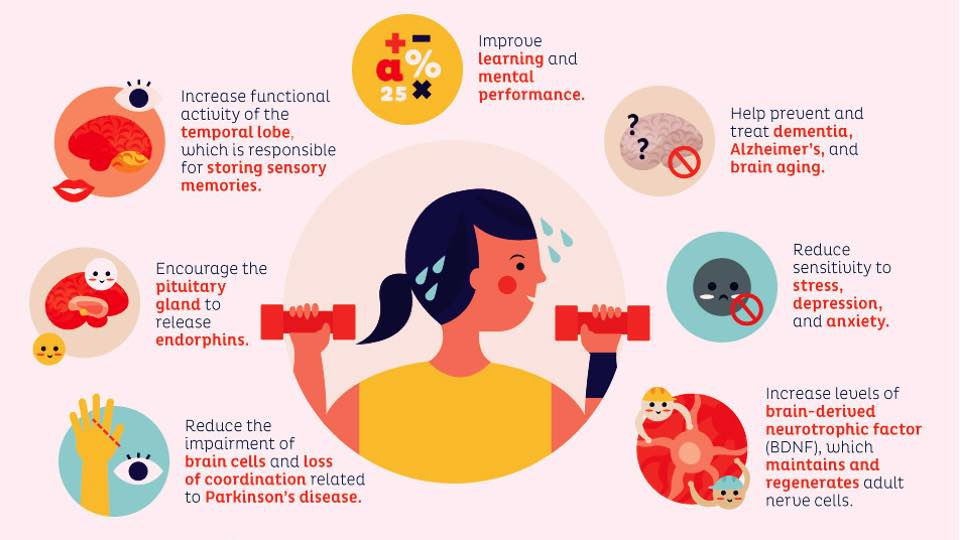 Exercise also seems to mimic some of the chemical effects of antidepressant medication. Based on increasing evidence, some scientists argue that certain cases of depression result from the impaired growth of both brain cells and the connections between them. Studies have documented the atrophy and loss of neurons in brain regions such as the amygdala, hippocampus and prefrontal cortex in patients with major depression. Antidepressants that increase levels of serotonin and other neurotransmitters might work by reinvigorating neural proliferation, a process that depends in part on a molecule called brain-derived neurotrophic factor (BDNF). In studies with both animals and people, exercise enhances the production of BDNF.
Exercise also seems to mimic some of the chemical effects of antidepressant medication. Based on increasing evidence, some scientists argue that certain cases of depression result from the impaired growth of both brain cells and the connections between them. Studies have documented the atrophy and loss of neurons in brain regions such as the amygdala, hippocampus and prefrontal cortex in patients with major depression. Antidepressants that increase levels of serotonin and other neurotransmitters might work by reinvigorating neural proliferation, a process that depends in part on a molecule called brain-derived neurotrophic factor (BDNF). In studies with both animals and people, exercise enhances the production of BDNF. Despite the mounting evidence that exercise can remedy some forms of depression, skepticism persists in academia and health care. Trivedi has found that there is a general bias that exercise is not a bona fide treatment—it’s just something you should do in addition to treatment, like trying to sleep and eat well. Even though recognition of exercise as a treatment is increasing, only some health insurance companies pay for gym time, and when they do, they often offer small temporary discounts.
Despite the mounting evidence that exercise can remedy some forms of depression, skepticism persists in academia and health care. Trivedi has found that there is a general bias that exercise is not a bona fide treatment—it’s just something you should do in addition to treatment, like trying to sleep and eat well. Even though recognition of exercise as a treatment is increasing, only some health insurance companies pay for gym time, and when they do, they often offer small temporary discounts.

 Studies confirm that many modern employees, are perpetually preoccupied with work: even when they get a break, they feel obligated to keep working. The European Union mandates 20 days of paid holiday, but the U.S. has no federal laws guaranteeing paid time off, sick leave or breaks for national holidays. Canada, Japan and Hong Kong mandate just 10 or fewer days of annual holidays; in the U.S., workers receive an average of just eight days after one year on the job. But a 2014 survey by Harris Interactive found that Americans use only half of their eligible holiday days and paid time off. A 2015 report by Expedia showed that Americans collectively neglect 1.3 million years of vacation annually. And in several surveys, U.S. workers have confessed that they do not fully unplug from phone or email even when they are on holiday or ill. The Americans are not alone when it comes to this.
Studies confirm that many modern employees, are perpetually preoccupied with work: even when they get a break, they feel obligated to keep working. The European Union mandates 20 days of paid holiday, but the U.S. has no federal laws guaranteeing paid time off, sick leave or breaks for national holidays. Canada, Japan and Hong Kong mandate just 10 or fewer days of annual holidays; in the U.S., workers receive an average of just eight days after one year on the job. But a 2014 survey by Harris Interactive found that Americans use only half of their eligible holiday days and paid time off. A 2015 report by Expedia showed that Americans collectively neglect 1.3 million years of vacation annually. And in several surveys, U.S. workers have confessed that they do not fully unplug from phone or email even when they are on holiday or ill. The Americans are not alone when it comes to this. In a survey of more than 300 part- or full-time workers published last year in the Journal of Occupational Health Psychology, Barber and her colleagues found that employees who reported greater workplace telepressure missed more days of work, experienced more physical and mental burnout, and did not sleep as well as their less email-obsessed peers. Barber also found that telepressure can lower the quality of an employee’s work: responsivity doesn’t always mean productivity – all it shows is that someone is responding and available, but that is different from doing good work.
In a survey of more than 300 part- or full-time workers published last year in the Journal of Occupational Health Psychology, Barber and her colleagues found that employees who reported greater workplace telepressure missed more days of work, experienced more physical and mental burnout, and did not sleep as well as their less email-obsessed peers. Barber also found that telepressure can lower the quality of an employee’s work: responsivity doesn’t always mean productivity – all it shows is that someone is responding and available, but that is different from doing good work. Changes to the brain’s structure and to behaviour most likely explain these improvements. Over time expert meditators may develop a more intricately wrinkled cortex—the brain’s outer layer, which is critical for many sophisticated mental abilities, such as abstract thought. These practitioners may also have increased volume and density in the hippocampus, an area that is absolutely crucial for memory. Finally, meditation appears to thicken regions of the frontal cortex that we rely on to regulate our emotions and prevent the typical wilting of brain areas responsible for sustaining attention as we age.
Changes to the brain’s structure and to behaviour most likely explain these improvements. Over time expert meditators may develop a more intricately wrinkled cortex—the brain’s outer layer, which is critical for many sophisticated mental abilities, such as abstract thought. These practitioners may also have increased volume and density in the hippocampus, an area that is absolutely crucial for memory. Finally, meditation appears to thicken regions of the frontal cortex that we rely on to regulate our emotions and prevent the typical wilting of brain areas responsible for sustaining attention as we age.


 Picture two female chimpanzees hanging out under a tree. One grooms the other, systematically working long fingers through fur, picking out bugs and bits of leaves. The recipient sprawls sleepily on the ground, looking as relaxed as someone enjoying a spa day. A subsequent surreptitious measurement of her levels of oxytocin, a hormone associated with bonding and pleasure, would confirm that she is pretty happy.
Picture two female chimpanzees hanging out under a tree. One grooms the other, systematically working long fingers through fur, picking out bugs and bits of leaves. The recipient sprawls sleepily on the ground, looking as relaxed as someone enjoying a spa day. A subsequent surreptitious measurement of her levels of oxytocin, a hormone associated with bonding and pleasure, would confirm that she is pretty happy. To most of us, the pleasures of friendship are familiar. Like this pair of chimps, we are more likely to relax and enjoy ourselves at dinner with people we know well than with people we have just met. Philosophers have celebrated the joys of social connection since the time of Plato, who wrote a dialogue on the subject, and there has been evidence for decades that social relationships are good for us. But it is only now that friendship is getting serious scientific respect. Researchers from disciplines as diverse as neurobiology, economics and animal behaviour are recognising parallels between the interactions of animals and the habits of people at dinner parties and are asking far more rigorous questions about the motivations behind social behaviour.
To most of us, the pleasures of friendship are familiar. Like this pair of chimps, we are more likely to relax and enjoy ourselves at dinner with people we know well than with people we have just met. Philosophers have celebrated the joys of social connection since the time of Plato, who wrote a dialogue on the subject, and there has been evidence for decades that social relationships are good for us. But it is only now that friendship is getting serious scientific respect. Researchers from disciplines as diverse as neurobiology, economics and animal behaviour are recognising parallels between the interactions of animals and the habits of people at dinner parties and are asking far more rigorous questions about the motivations behind social behaviour. Most critically, friendship is sustained. You might have a pleasant interaction with someone on the subway but would not call that person your friend. But the neighbour with whom you regularly exercise and occasionally dine? That is a friend.
Most critically, friendship is sustained. You might have a pleasant interaction with someone on the subway but would not call that person your friend. But the neighbour with whom you regularly exercise and occasionally dine? That is a friend. Christakis joined forces with James Fowler, a political scientist now at the University of California, San Diego (both were then at Harvard University), to study social networks of 3,000 or 30,000 or more people. Using computational techniques, they and others have established measures of connectedness that allow sophisticated mapping of these bonds. For example, they count how many friends I would name (“out-degree”) and how many friends name me (“in-degree”) separately—thereby dealing with any mismatch in our perceptions of how close we really are. Their 2009 book, Connected: The Surprising Power of Our Social Networks and How They Shape Our Lives, made the case that social connections of up to three degrees of separation have a significant influence on such things as weight as well as on smoking habits, altruism and voting behaviours.
Christakis joined forces with James Fowler, a political scientist now at the University of California, San Diego (both were then at Harvard University), to study social networks of 3,000 or 30,000 or more people. Using computational techniques, they and others have established measures of connectedness that allow sophisticated mapping of these bonds. For example, they count how many friends I would name (“out-degree”) and how many friends name me (“in-degree”) separately—thereby dealing with any mismatch in our perceptions of how close we really are. Their 2009 book, Connected: The Surprising Power of Our Social Networks and How They Shape Our Lives, made the case that social connections of up to three degrees of separation have a significant influence on such things as weight as well as on smoking habits, altruism and voting behaviours. Research in animals has been important in establishing the idea that a strong social bond—all by itself—may have evolutionary significance. Evolutionary theories are hard to prove. Many experiments designed to test these ideas require studying not just a single group or population but their descendants. Most animal species have shorter life spans than humans, however, making measuring generational change a simpler proposition. That can make it easier to tease out cause from correlation. In addition, findings that echo across species suggest biological rather than cultural origins. To date, horses, elephants, hyenas, monkeys, chimpanzees, whales and dolphins have all been shown to form social bonds that can last for years. Studies of our closest living relatives— monkeys and apes—have been especially groundbreaking. Seyfarth and Cheney have studied the same troop of baboons in Kenya for more than 30 years. When they began, primatologist Robert Hinde had already established that nonhuman primates had notable social relationships. One of the first things Seyfarth and Cheney did was use audio-playback experiments to show that baboons were aware of the relationships of others. When a group of female monkeys heard an offspring’s distress vocalisation, they often looked at the infant’s mother. That suggests that the social relationships were not just a figment of our human imagination.
Research in animals has been important in establishing the idea that a strong social bond—all by itself—may have evolutionary significance. Evolutionary theories are hard to prove. Many experiments designed to test these ideas require studying not just a single group or population but their descendants. Most animal species have shorter life spans than humans, however, making measuring generational change a simpler proposition. That can make it easier to tease out cause from correlation. In addition, findings that echo across species suggest biological rather than cultural origins. To date, horses, elephants, hyenas, monkeys, chimpanzees, whales and dolphins have all been shown to form social bonds that can last for years. Studies of our closest living relatives— monkeys and apes—have been especially groundbreaking. Seyfarth and Cheney have studied the same troop of baboons in Kenya for more than 30 years. When they began, primatologist Robert Hinde had already established that nonhuman primates had notable social relationships. One of the first things Seyfarth and Cheney did was use audio-playback experiments to show that baboons were aware of the relationships of others. When a group of female monkeys heard an offspring’s distress vocalisation, they often looked at the infant’s mother. That suggests that the social relationships were not just a figment of our human imagination.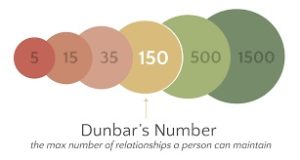 If evolution is steering various species, including our own, toward prosocial behaviour, it makes sense to seek evidence in the genome. Already genetic variation has been identified in people with disorders that affect social function, such as autism and schizophrenia. And some genes in the dopamine and serotonin pathways have been consistently linked with social traits. Genetics started with an understanding of how genes affect the structure and function of our bodies and then our minds. And now scientists are beginning to ask how genes affect the structure and function of our societies.
If evolution is steering various species, including our own, toward prosocial behaviour, it makes sense to seek evidence in the genome. Already genetic variation has been identified in people with disorders that affect social function, such as autism and schizophrenia. And some genes in the dopamine and serotonin pathways have been consistently linked with social traits. Genetics started with an understanding of how genes affect the structure and function of our bodies and then our minds. And now scientists are beginning to ask how genes affect the structure and function of our societies. As part of this work, in a 2012 paper in Nature, they even mapped the social network of the Hadza hunter-gatherers of Tanzania, who live essentially as humans did 10,000 years ago. Christakis and Fowler showed that the Hadza form networks with a mathematical structure just like humans living in modernised settings, suggesting something very fundamental about the structure of friendship.
As part of this work, in a 2012 paper in Nature, they even mapped the social network of the Hadza hunter-gatherers of Tanzania, who live essentially as humans did 10,000 years ago. Christakis and Fowler showed that the Hadza form networks with a mathematical structure just like humans living in modernised settings, suggesting something very fundamental about the structure of friendship. But of course, the most straightforward result of this work would be to spark a deeper appreciation of just how important our friends are in our life. Other individuals are in fact the source of some of our greatest joys. And now we know that they do not just make us happy—they help keep us alive. So time to celebrate the power and inportance of your friendships for the rest of this year – and well on into the future!
But of course, the most straightforward result of this work would be to spark a deeper appreciation of just how important our friends are in our life. Other individuals are in fact the source of some of our greatest joys. And now we know that they do not just make us happy—they help keep us alive. So time to celebrate the power and inportance of your friendships for the rest of this year – and well on into the future!
 Researchers at the University of Texas at Austin put together a speed-dating pool of about 200 men and women. They also took photos of the participants, mimicking those found on online dating sites, and recorded short videos of the same individuals to see what kinds of first impressions people would form in each context. For each scenario, participants rated those they “met” on traits such as attractiveness, humour, intelligence and other qualities that we usually judge within seconds. The researchers presented their findings in January at the Society for Personality and Social Psychology meeting in San Diego.
Researchers at the University of Texas at Austin put together a speed-dating pool of about 200 men and women. They also took photos of the participants, mimicking those found on online dating sites, and recorded short videos of the same individuals to see what kinds of first impressions people would form in each context. For each scenario, participants rated those they “met” on traits such as attractiveness, humour, intelligence and other qualities that we usually judge within seconds. The researchers presented their findings in January at the Society for Personality and Social Psychology meeting in San Diego. In another new paper, in the Journal of Experimental Social Psychology, researchers asked whether contrast effects occur when judging personality. Participants viewed two dating profiles. When the first person came across as uncaring (“I get bored talking about feelings and stuff”), the second person, who was nice but unattractive, seemed much more appealing. In real profiles, people might not appear as blatantly callous as in this study, but other personality traits could be turnoffs that bias viewers’ later decisions.
In another new paper, in the Journal of Experimental Social Psychology, researchers asked whether contrast effects occur when judging personality. Participants viewed two dating profiles. When the first person came across as uncaring (“I get bored talking about feelings and stuff”), the second person, who was nice but unattractive, seemed much more appealing. In real profiles, people might not appear as blatantly callous as in this study, but other personality traits could be turnoffs that bias viewers’ later decisions. The researchers selected 100,000 users of a large online dating site and gave half of them the ability to browse anonymously, which usually costs extra. They became less inhibited and more likely to look at people of the same sex or a different race. The researchers thought the disinhibition would translate into more matches….but….women with this ability actually made fewer matches because they did not leave so-called weak signals of interest that might lead the other party to follow up. The simple notification that a particular person perused your profile is often enough to get a conversation started. Anonymous browsing did not affect men’s matches as much, because the men were already uninhibited—they messaged individuals who interested them. Women, however, are less likely in general to make the first move and therefore depend more on sending weak signals to invite flirtation.
The researchers selected 100,000 users of a large online dating site and gave half of them the ability to browse anonymously, which usually costs extra. They became less inhibited and more likely to look at people of the same sex or a different race. The researchers thought the disinhibition would translate into more matches….but….women with this ability actually made fewer matches because they did not leave so-called weak signals of interest that might lead the other party to follow up. The simple notification that a particular person perused your profile is often enough to get a conversation started. Anonymous browsing did not affect men’s matches as much, because the men were already uninhibited—they messaged individuals who interested them. Women, however, are less likely in general to make the first move and therefore depend more on sending weak signals to invite flirtation.