It all began with a cough.
Three years ago Tracey, a Scottish woman in her mid-30s, caught a bad chest infection that left her with a persistent cough that refused to subside, even after medication. A few months later strange symptoms started to appear. She noticed numbness spreading through her legs and began to feel that their movement was out of her control. When she walked, she felt like a marionette, with someone else pulling the strings. Over the course of two weeks the odd loss of sensation progressively worsened. Then, one evening at home, Tracey’s legs collapsed beneath her. She lay there, feeling like she couldn’t breathe. Unable to feel anything below her waist, her mother rushed her to the hospital where she then remained for more than half a year.
During her first few weeks in the hospital, Tracey endured a barrage of tests as doctors tried to uncover the cause of her symptoms. It could be a progressive neurodegenerative condition such as motor neuron disease, they thought. Or maybe it was multiple sclerosis, a disease in which the body’s own immune cells attack the nervous system. Bafflingly, however, the brain scans, blood tests, spinal taps and everything else came back normal.
 Tracey’s predicament is not uncommon. According to one of the most comprehensive assessments of neurology clinics to date, roughly a third of patients have neurological symptoms that are deemed to be either partially or entirely unexplained. These may include tremour, seizures, blindness, deafness, pain, paralysis and coma and can parallel those of almost any neurological disease. In some patients, such complications can persist for years or even decades; some people require wheelchairs or cannot get out of bed. Although women are more often diagnosed than men, such seemingly inexplicable illness can be found in anyone and across any life span.
Tracey’s predicament is not uncommon. According to one of the most comprehensive assessments of neurology clinics to date, roughly a third of patients have neurological symptoms that are deemed to be either partially or entirely unexplained. These may include tremour, seizures, blindness, deafness, pain, paralysis and coma and can parallel those of almost any neurological disease. In some patients, such complications can persist for years or even decades; some people require wheelchairs or cannot get out of bed. Although women are more often diagnosed than men, such seemingly inexplicable illness can be found in anyone and across any life span.
Generations of scientists have tried to understand these bizarre conditions, which have historically been given diverse names, such as hysteria, conversion disorder or psychosomatic illness. These labels have, however, long imposed particular explanations for what many researchers now regard as a complex illness at the interface of psychiatry and neurology. Some are still in use today, but the newest name for these conditions, functional neurological disorder(FND), is deliberately neutral, simply denoting a problem in the functioning of the nervous system.
Patients with FND have long struggled to obtain adequate care. They have been accused of feigning or imagining symptoms, painfully but often fruitlessly probed for childhood trauma and dismissed by doctors who did not know how to treat someone who, based on all the usual tests, appeared to be healthy. For many, many years physicians have underestimated the prevalence of these disorders and the human toll it takes. These people have really fallen in the gap between the fields of neurology and psychiatry.
Over the past decade or so, however, using techniques such as functional magnetic resonance imaging (fMRI), researchers have begun to understand what happens in the brains of patients with this enigmatic illness. And by applying new models of how the brain works, they are gaining a better understanding of how the condition arises and how it may be treated.
ENIGMATIC ILLNESSES
More than 3,000 years ago Mursili II, king of the Hittites, was caught in a terrifying thunderstorm. The experience left him with a temporary speech impediment that went away—only to return several years later, after the monarch woke from a nightmare about the incident. His subjects attributed their king’s curious ailment to the wrath of the Storm God, one of the most important deities of the ancient civilization. When modern-day scholars revisited the documents detailing the event, they interpreted it as functional aphonia (the inability to speak).
Like the Hittites, people throughout history have turned to the supernatural—gods, witchcraft and demonic possession—to explain illnesses that today would likely be diagnosed as FND. According to some historical interpretations, the first scientific attempt to account for them emerged around 400 B.C.E., when Greek physicians, including Hippocrates, coined the term “hysteria” to describe a wide collection of ailments, among them paralysis, headaches, dizziness and pain, in the belief that they were caused by the uterus (hystera, in Greek) wandering about the body.
 Hysteria had its heyday in the 19th century, when it moved from the womb to the brain. Among several physicians who studied it was Jean-Martin Charcot, regarded by many as the “father of neurology.” At the Salpêtrière Hospital in Paris, he painstakingly detailed the symptoms of patients with hysteria and, after they died, conducted autopsies on their brains. Although Charcot was unable to identify any structural aberrations in those subjects, he was convinced that the impairments he saw were associated with unobservable, fluctuating changes in the brain, which he called “dynamic or functional lesions.”
Hysteria had its heyday in the 19th century, when it moved from the womb to the brain. Among several physicians who studied it was Jean-Martin Charcot, regarded by many as the “father of neurology.” At the Salpêtrière Hospital in Paris, he painstakingly detailed the symptoms of patients with hysteria and, after they died, conducted autopsies on their brains. Although Charcot was unable to identify any structural aberrations in those subjects, he was convinced that the impairments he saw were associated with unobservable, fluctuating changes in the brain, which he called “dynamic or functional lesions.”
Charcot also discovered that, contrary to common belief, male hysteria was not rare; instead it often went undetected. He highlighted, for example, cases of hysteria among workers at a national railway company that had seemingly emerged after minor physical injuries. His work popularised the study of hysteria, inspiring several researchers, including Joseph Babinski, Pierre Janet and Sigmund Freud, to investigate it as well.
Unlike Charcot, however, these men viewed the condition as a disorder of the mind rather than the brain. Freud proposed that it arose when repressed trauma from childhood abuse or other disturbing events was transformed into physical symptoms; accordingly, he called it conversion disorder. That view and label cemented the displacement of the disorder from the realm of neurology to that of psychiatry and became the dogma for much of the 20th century. Perhaps coincidentally, as Freud’s influence in psychiatry faded over the decades, so did cases of conversion disorder—to the point where some viewed it as a bygone ailment of the Victorian era.
A century later a new generation of investigators has turned its attention to this condition. Careful observation of patients indicates that despite the drop in diagnoses in the latter half of the 1900s, these disorders have not disappeared. And new research reveals that the condition encompasses both neurology and psychiatry. In 2013 some physicians, concerned that the term “conversion disorder” was not widely accepted by patients and perhaps incorrectly pointed to psychology as an exclusive driver for the condition, lobbied for a change—causing FND to be included as an alternative name for the ailment in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
TELLTALE SIGNS
Jon Stone of the University of Edinburgh specialises in diagnosing and treating FND. Stone listens carefully as people describe when, where and how their symptoms started. He collects detailed information about their medical and personal histories and conducts a neurological examination. He listens. Then, like a detective, he pieces these details together to make a diagnosis.
 In recent years FND has gone from a diagnosis of exclusion—a label doctors reserved for patients whose conditions defied all other explanations—to one made after identifying distinct signs and symptoms. These resemble those of other neurological disorders but possess identifiable differences. One example is Hoover’s sign, in which weakness in a limb is temporarily corrected when the patient’s attention is directed elsewhere. Another is tremour entrainment: when patients with a functional tremour in one arm are asked to start shaking the other at a regular rhythm, the affected hand will start to shake with the same rhythm as the other. This effect does not occur in people with neurodegenerative conditions such as Parkinson’s disease. Clear signs of functional seizures include tightly shut eyes, rapid breathing and shaking that lasts for several minutes—features rarely seen during epileptic attacks.
In recent years FND has gone from a diagnosis of exclusion—a label doctors reserved for patients whose conditions defied all other explanations—to one made after identifying distinct signs and symptoms. These resemble those of other neurological disorders but possess identifiable differences. One example is Hoover’s sign, in which weakness in a limb is temporarily corrected when the patient’s attention is directed elsewhere. Another is tremour entrainment: when patients with a functional tremour in one arm are asked to start shaking the other at a regular rhythm, the affected hand will start to shake with the same rhythm as the other. This effect does not occur in people with neurodegenerative conditions such as Parkinson’s disease. Clear signs of functional seizures include tightly shut eyes, rapid breathing and shaking that lasts for several minutes—features rarely seen during epileptic attacks.
Such indicators have been known to doctors for decades—Hoover’s sign, for one, was observed by physician Charles Franklin Hoover in the 19th century. In the past, doctors (according to Stone) would hide such signs from patients. But he shows them to patients to help them understand the nature of their condition and notes that doctors are increasingly taking up this practice. Seeing such clues can help to grasp a condition that Stone likes to describe as a “software problem, not a hardware problem” in the brain.
Stone first came across these disorders as a junior doctor in the early 1990s. He found himself fascinated by them; having grown up with a stutter meant that he had experienced being unable to control his own body. And he was disturbed by how those with FND, as he prefers to call the condition, were being treated. The common attitude among medical professionals was that the symptoms were not real—at least not in the same way as those seen in multiple sclerosis or stroke, for example. Many physicians were concerned that they would either fail to identify the true cause of a patient’s illness or be fooled by someone faking their symptoms. As a result, patients with FND did not receive the same level of sympathy, attention or care as those with so-called organic neurological illnesses.
Stone decided to dig deeper. During his doctoral studies at the University of Edinburgh, he met Alan Carson, who was training to become a psychiatrist and shared his interest. In 2002 the pair began to assess the scale of the problem by following the referrals to four neurology centres in Scotland over a period of 15 months. Their examination, which included more than 3,700 patients, revealed that 1,144—close to a third—had neurological symptoms deemed as partially or completely medically unexplained. Of those, only four ended up being diagnosed with another neurological issue 18 months after their initial consultation. This work demonstrated how widespread these disorders were.
Eventually Stone and Carson joined forces with Mark Hallett, a neurologist at the National Institute of Neurological Disorders and Stroke in the U.S., who had also been taking strides to advance the field. In addition to conducting his own research, Hallett had begun mobilising a group of scientists and doctors who could contribute to the study of FND. The community gradually ballooned from several dozens of attendees at a small workshop to a full-blown society for FND, which was founded by Hallett, Carson and Stone and was inaugurated in 2019.
PREDICTIONS GONE AWRY
 A year after landing in the hospital because of her FND, Tracey was referred to a psychologist. At first, she did not think she needed to be there—her symptoms had been improving with physiotherapy. After several sessions of psychotherapy, however, she made a shocking discovery: she had blocked the memory of certain key events in her childhood. Among those forgotten experiences were years of physical abuse at the hands of a family friend.
A year after landing in the hospital because of her FND, Tracey was referred to a psychologist. At first, she did not think she needed to be there—her symptoms had been improving with physiotherapy. After several sessions of psychotherapy, however, she made a shocking discovery: she had blocked the memory of certain key events in her childhood. Among those forgotten experiences were years of physical abuse at the hands of a family friend.
Although she had initially been reluctant to consider the role of psychological factors in her illness, Tracey now says that she thinks they do contribute. Many of those who study FND today would agree—with caveats. Unlike Freud, who focused on the role of repressed trauma, researchers now recognise that myriad factors are associated with this condition. These include predisposing factors, such as adverse experiences during childhood, a previous physical injury or mood and anxiety disorders; triggers such as physical injury or a stressful life event; and maintaining factors, such as a lack of access to proper treatment or a patient’s responses to and beliefs about the condition. The leading framework for thinking about FND, the so-called biopsychosocial model, takes all these factors into account.
As yet, there is no single, widely accepted explanation for how these influences come together to create FND, but some scientists have suggested that the malady involves arguably one of the most fundamental functions of the brain: predictive processing. Championed by neuroscientist Karl Friston of University College London, predictive processing posits that the brain is constantly making and evaluating predictions by comparing the data generated from our sensory organs to internal models built from previous experience. When mismatches occur between inferences and reality, the brain either updates its existing models or sends commands back down to the body to act in ways that align with our expectations. For instance, if you want to walk, but your leg is not moving, the brain will generate a prediction error that can be resolved if you move that leg. In this way, Friston and others propose, predictions underlie everything the brain does, from perception to movement to decision-making.
Neurologist Mark Edwards of St. George’s University Hospital in London and his colleagues have suggested that with FND, this predictive machinery goes awry, so that patients develop abnormal inferences of how their body should feel or function. One of the biggest drivers of this anomaly, according to Edwards, is excessive focus on one’s own body. This heightened attention can be attributed to a variety of factors, including an existing physical illness, mood and anxiety disorders, or childhood abuse. When a person experiences a triggering event—say, an injury to a limb or a panic attack—this heightened attentiveness may drive one’s brain to develop altered predictions about the body. In some cases, a past experience, such as exposure to sickness in the family, might also help shape these expectations.
 Consider someone who falls and badly sprains a leg, resulting in a temporary loss of mobility in that limb. In most people, the brain’s predictions about the injured leg’s ability to move would get updated once mobility returns. This person, however, has a tendency toward mild anxiety that amplifies the levels of subconscious attention they pay to their body and has been sensitive to health events since the sudden death of a parent. These predisposing factors magnify the sensations associated with injury; in consequence, the internal model of the immobile leg persists even after the limb regains its function, leading to functional paralysis. (In some ways, this is the opposite of what happens in people who experience phantom limb syndrome. Those people are unable to update the prediction error that occurs when an expected sensation in a missing limb is not met with actual sensory feedback.)
Consider someone who falls and badly sprains a leg, resulting in a temporary loss of mobility in that limb. In most people, the brain’s predictions about the injured leg’s ability to move would get updated once mobility returns. This person, however, has a tendency toward mild anxiety that amplifies the levels of subconscious attention they pay to their body and has been sensitive to health events since the sudden death of a parent. These predisposing factors magnify the sensations associated with injury; in consequence, the internal model of the immobile leg persists even after the limb regains its function, leading to functional paralysis. (In some ways, this is the opposite of what happens in people who experience phantom limb syndrome. Those people are unable to update the prediction error that occurs when an expected sensation in a missing limb is not met with actual sensory feedback.)
The hypothesis that predictive processing is altered in FND patients has now been tested in a handful of experiments. In a 2014 study, for example, Edwards and his team used a task called force matching, in which a robotic device presses down on a finger and people are asked to match the force with their own hand. Healthy people tend to overestimate the force required by their own hand because the brain’s expectations “cancel out” some of its force (a similar explanation applies to why you cannot tickle yourself). People with FND, on the other hand, were abnormally accurate, indicating that the internal prediction system was functioning differently. Even so, much more evidence is needed to prove that this mechanism provides a correct and sufficient explanation for the condition.
PROBING THE BRAIN
Like Charcot, contemporary investigators of FND have been examining the brains of patients to find changes associated with the condition. Modern scientists, however, no longer have to wait to conduct an autopsy to peer into their subjects’ skulls. Using techniques such as fMRI, researchers have begun to reveal there are indeed differences in the brains of individuals with FND. They are beginning to identify the dynamic lesion that Charcot was looking for all those years ago.
With fMRI, researchers have identified distinct patterns of activity in brain areas such as the temporoparietal junction—associated with a sense of agency—in those with FND, compared with those asked to mimic the same symptoms. These findings help to confirm that unlike conditions such as factitious disorder (a severe form of which is known as Munchausen syndrome), in which patients deliberately act out other illnesses, symptoms in individuals with FND are out of their control.
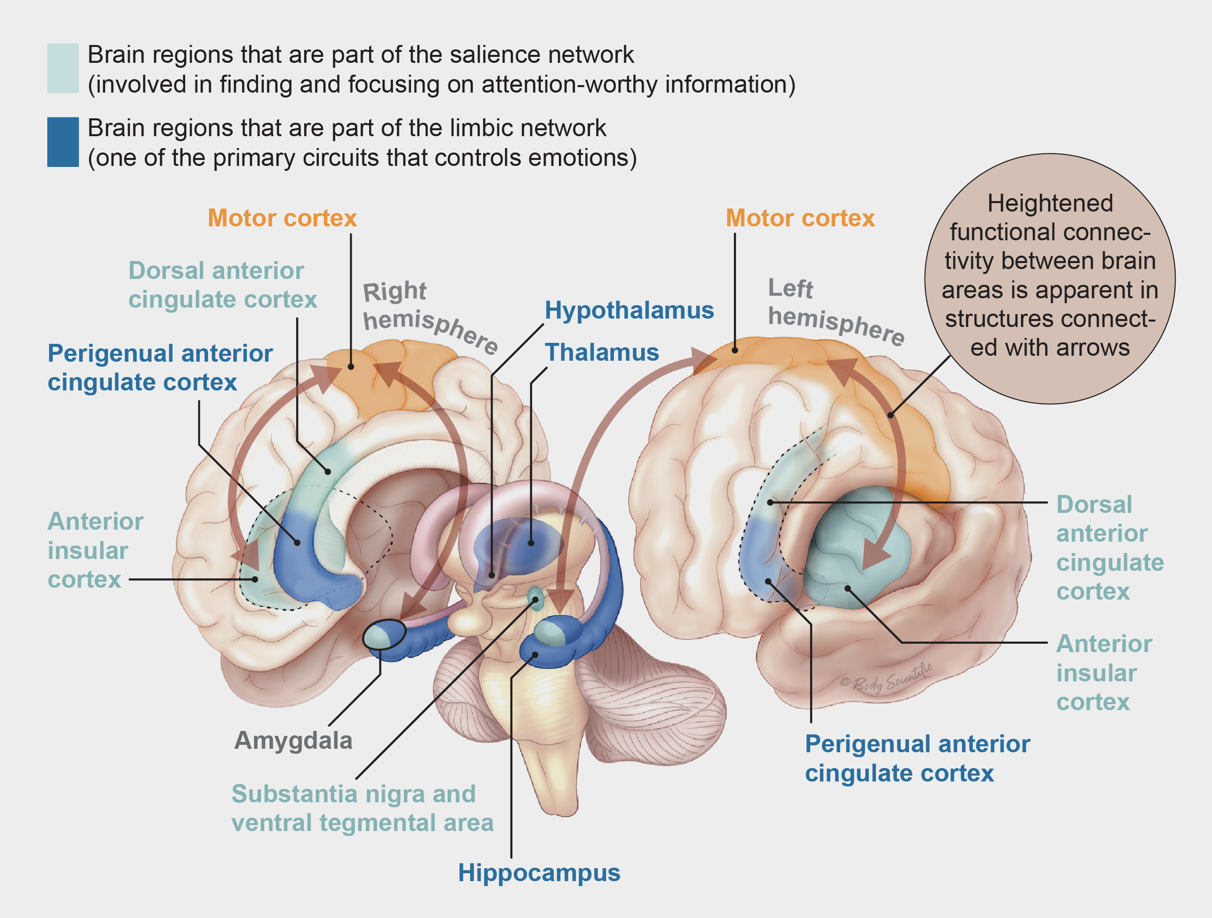
Another significant discovery from neuroimaging is that people with FND have enhanced connectivity between the motor-control regions and two brain networks involved in emotional processing: the salience network, responsible for detecting and focusing on attention-worthy information, and the limbic network, one of the primary systems controlling emotion. In a 2010 study, for example, Hallett’s group reported heightened linkages between the amygdala, a key region in the limbic system, and the supplementary motor area, which is responsible for preparing to initiate movements. Others, such as David Perez, a neurologist-psychiatrist at Massachusetts General Hospital, have shown hyperconnectivity between motor regions and salience network areas such as the insula and the anterior cingulate. These observations suggest that, at least in a subset of people with FND, the emotional circuitry might be hijacking the motor system.
Perez’s team has also found that some risk factors may map onto these circuits. In a study published this year, his group reported that the magnitude of the coupling of the motor regions with the limbic and salience areas of the brain positively correlated with the degree to which patients experienced physical abuse during childhood. Perez emphasises, however, that this will probably be relevant only to the subset of patients in whom trauma is present: in his study, a significant proportion of patients did not report any childhood physical abuse. Still, he notes that these findings point to how a risk factor such as trauma could alter brain circuits in people who develop FND.
Scientists are also investigating how factors such as stress alter brain circuits in FND. Neurologist Selma Aybek of the University of Bern says that although not all patients have a history of trauma or stress, they may possess differences in their biological stress response. Her group has found that, compared with healthy individuals, FND patients have higher levels of the stress markers cortisol and amylase and report being more stressed after taking part in a stressful task. Building on these findings, her team is using neuroimaging to examine whether there is an association between stress-related regions and agency-related regions in FND patients’ brains.
Thus, a picture of the pathophysiology of FND patients is slowly emerging. But most of this work has been conducted in patients with motor symptoms, which means that sensory symptoms such as altered vision have yet to be explored. Many of these studies also have had small sample sizes, so findings will need to be validated in larger trials. How these neuroimaging findings fit with the predictive-processing model also remains an open question. It is plausible, Perez notes, that many of the areas identified so far may be the circuitry through which the altered predictions arise.
A BRIGHTER FUTURE
In the summer after her second year of teacher’s college in Scotland, a 19-year-old woman named Rachael Troup was rushed to the hospital with what appeared to be a stroke. Brain scans showed that she did not have a stroke, however, and tests for other neurological diseases came back normal. Eventually Troup was diagnosed with FND. But when she started treatment, it was excruciating. Neither her doctors nor her physiotherapists seemed to know much about how to treat her condition, and the exercises they made her do hurt more than they helped.
 After a few months Troup decided to stop going to physiotherapy. At the time the entire right side of her body was barely functioning, and she was using a wheelchair for mobility. After being admitted to the hospital several more times for strokelike attacks, however, Troup met Stone’s team and was provided with FND-tailored care. It involved a form of physiotherapy that employs techniques such as distraction to shift the spotlight of attention away from the affected limbs while engaging in exercises to help restore normal control.
After a few months Troup decided to stop going to physiotherapy. At the time the entire right side of her body was barely functioning, and she was using a wheelchair for mobility. After being admitted to the hospital several more times for strokelike attacks, however, Troup met Stone’s team and was provided with FND-tailored care. It involved a form of physiotherapy that employs techniques such as distraction to shift the spotlight of attention away from the affected limbs while engaging in exercises to help restore normal control.
For FND patients, shifting focus away from affected limbs is often a crucial part of physiotherapy because, as Edwards’s predictive-processing model suggests, attention is critical to the generation of symptoms. With attention deployed elsewhere, the brain’s abnormal expectations about movement are unable to take hold. Stone and his colleagues are part of an ongoing U.K.-wide, randomised controlled clinical trial testing this type of specialised physiotherapy for functional motor disorders (a subset of FND affecting movement). In addition to retraining movement, the treatment includes educating patients about how such symptoms could arise and the physical and psychological factors that may underlie it.
To expand the tool kit of interventions for FND, researchers are also testing other alternatives. Another large clinical trial with more than 300 patients assessed the efficacy of cognitive-behavioral therapy (CBT)—a type of goal-oriented intervention focused on changing disruptive patterns of thinking or behavior—for functional seizures. The findings, published in June in Lancet Psychiatry, suggest that CBT may not reduce seizure frequency in all patients.
At King’s College London, neuropsychiatrist Tim Nicholson and his team are examining a noninvasive method of exciting the brain known as transcranial magnetic stimulation (TMS) as a potential intervention for FND. His group recently completed a feasibility study, and the results were promising enough to initiate a larger pilot clinical trial. There are competing explanations for why TMS might work. It induces a brief muscle twitch that could kickstart the relearning of movement; stimulating brain areas altered in FND might help restore function, or it may have a placebo effect. LaFaver’s group at Northwestern is examining the use of meditation and mindfulness practice, which, according to LaFaver, patients have anecdotally reported as helpful for maintaining the benefits of treatment.
Psychological treatments such as CBT currently remain among the first-line interventions for people with FND, according to Perez. There is a pressing need for a range of effective treatments, however: the prognosis remains poor. It is still relatively uncommon for FND patients to completely regain function, and relapses occur often. According to a 2014 meta-analysis of 24 studies, on average 40 percent of patients reported similar or worsened symptoms seven years after their initial diagnosis. On top of that, patients still experience high levels of stigma and have trouble accessing treatment.
Fortunately, the situation is changing. As researchers’ interest in FND surged over the past decade, so did the number of FND clinics around the world. Patients are speaking up as well. In 2012, for example, the international charity FND Hope was established with the aim of raising awareness and empowering patients.
Still, debates linger—and are reflected in an ongoing tussle over the name of the illness. In what fraction of patients are psychological factors present, for example? Do symptoms primarily arise through conversion of stressors, or are other explanations also necessary? One meta-analysis found that reports of stressors in FND patients vary between 23 and 86 percent in different studies. W. Curt LaFrance, Jr., a neurologist-psychiatrist at Brown University, says that it takes more time to identify such stressors than some doctors can devote to an individual patient—which may account for this enormous spread. In his clinic and in the scientific literature, he has consistently seen evidence of psychological stressors having converted into physical symptoms, and, accordingly, he supports use of the term “conversion disorder.” Partially reflecting such views, the older name remained when FND was added to the DSM-5, but the need to identify psychological factors for a diagnosis was dropped. That removal also remains contentious.
One thing is clear, however: because the condition lies at the crossroads of neurology and psychiatry, insights from both fields will be necessary to solve the puzzle. This blurring of the line between mental and physical illness is a growing trend. Scientists now understand, for example, that stress—a psychological factor—can predispose people to Alzheimer’s disease and that inflammation—a physical factor—may give rise to depression. In addition, traditional neurological diseases such as epilepsy and stroke are often associated with mood and behavioural disturbances.
Over the past few years Tracey, who started off the article this month, has frequently used a wheelchair because of her FND. But with the help of both physiotherapy and psychotherapy, she has started to recover. Her symptoms are not gone—she still experiences a lack of sensation in her legs, altered vision and pain—and some days are worse than others. She constantly feels like she’s fighting against her body, but she hopes to make a full recovery.
Maybe it’s obvious but the brain doesn’t separate into neurology and psychiatry. Perhaps what we actually need is a new science of brain and mind that really encapsulates that brain health equals mental health and physical health.
REFERENCES:
Jon Stone et al. Symptoms ‘unexplained by organic disease’ in 1144 new neurology out-patients: how often does the diagnosis change at follow-up? Brain, Volume 132, Issue 10, October 2009, pages 2878–2888.
Mark J. Edwards et al. A Bayesian account of ‘hysteria’. Brain. 2012 Nov; 135 (Pt 11) pages 3495-3512.
Isabel Parées et al. Loss of sensory attenuation in patients with functional (psychogenic) movement disorders. Brain, Volume 137, Issue 11, November 2014, Pages 2916–2921.
Valerie Voon et al. The involuntary nature of conversion disorder. Neurology. January 19, 2010, 74 (3).
Susannah Pick et al. Emotional Processing in Functional Neurological Disorder: A Review, Biopsychosocial Model and Research Agenda. Journal of Neurology, Neurosurgery and Psychiatry, Vol. 90; 2019.
Valerie Voon et al. Emotional stimuli and motor conversion disorder. Brain. 2010 May;133(Pt 5), 1526-1536.
Diana Kwon. Decoding a Disorder at the Interface of Mind and Brain. Scientific American. November 1, 2020.
Ibai Diez et al. Early-life trauma endophenotypes and brain circuit–gene expression relationships in functional neurological (conversion) disorder. Molecular Psychiatry. 2020. https://doi.org/10.1038/s41380-020-0665-0
Kalliopi Apazoglou et al. Biological and perceived stress in motor functional neurological disorders. Psychoneuroendocrinology. 2017 Nov, 85, pages 142-150.
Laura H. Goldstein et al. Cognitive behavioural therapy for adults with dissociative seizures (CODES): a pragmatic, multicentre, randomised controlled trial. Lancet Psychiatry. Vol. 7, issue 6, pages 491-505.
Jeannette Gelauff et al. The prognosis of functional (psychogenic) motor symptoms: a systematic review. J. Neurol Neurosurg Psychiatry. 2014 Feb, 85(2), pages 220-226.
Lea Ludwig et al. Stressful life events and maltreatment in conversion (functional neurological) disorder: systematic review and meta-analysis of case-control studies. Lancet Psychiatry. Vol. 5, issue 4, pages 307-320.

 There are both passive and active forms of physical rest.
There are both passive and active forms of physical rest. Next up is mental rest—who doesn’t need some of that with all of the stress we have in our lives and with the covid pandemic! Mental fatigue can result from a variety of things including negative self-talk, over-thinking, anxious what-if thinking, being stuck in the past, and judgements.
Next up is mental rest—who doesn’t need some of that with all of the stress we have in our lives and with the covid pandemic! Mental fatigue can result from a variety of things including negative self-talk, over-thinking, anxious what-if thinking, being stuck in the past, and judgements. One way to ease the mental load is through use of good time management skills. Remember to take into account not only the amount of time the task takes, but the emotional load of the task as well. There are things that we do that may not take that much time, but we will need time before or after the event due to the strain on our minds or emotions. For example, spending 1 hour folding the washing is different from spending 1 hour caring for an ill family member. The effective time for the family member activity might be
One way to ease the mental load is through use of good time management skills. Remember to take into account not only the amount of time the task takes, but the emotional load of the task as well. There are things that we do that may not take that much time, but we will need time before or after the event due to the strain on our minds or emotions. For example, spending 1 hour folding the washing is different from spending 1 hour caring for an ill family member. The effective time for the family member activity might be The first step in getting more emotional rest is being mindful of your environment. Emotions are contagious! Are you around people who complain all the time or are judgmental? As best you can, modify these environments by removing unnecessary negativity and coping ahead for when you have to be in stressful situations.
The first step in getting more emotional rest is being mindful of your environment. Emotions are contagious! Are you around people who complain all the time or are judgmental? As best you can, modify these environments by removing unnecessary negativity and coping ahead for when you have to be in stressful situations. Another thing that is helpful in reducing the amount of (social) comparisons that you do. You probably wouldn’t be surprised that many of us engage in emotionally draining comparisons several times a day. Are you scrolling through social media, comparing your looks, your skills, and your furniture choices to those you see on Facebook and Instagram? Stop it, it’s creating more of a deficit for you.
Another thing that is helpful in reducing the amount of (social) comparisons that you do. You probably wouldn’t be surprised that many of us engage in emotionally draining comparisons several times a day. Are you scrolling through social media, comparing your looks, your skills, and your furniture choices to those you see on Facebook and Instagram? Stop it, it’s creating more of a deficit for you. Spirituality is broad. It can include organised religious practices, but spiritual rest can simply be about connecting with something greater than yourself. It could include prayer or a spiritual practice. But basically anything that gives you a sense of belonging, a sense of purpose and feeling connected to that ‘something bigger’ means you’re on the right track.
Spirituality is broad. It can include organised religious practices, but spiritual rest can simply be about connecting with something greater than yourself. It could include prayer or a spiritual practice. But basically anything that gives you a sense of belonging, a sense of purpose and feeling connected to that ‘something bigger’ means you’re on the right track. But do remember that your social circles – be it a club, a group of friends or a team sport – help to deepen relationships and make you feel more connected. People are dynamic and it’s important to embrace all of your social needs. Whatever you’re into, there is a group of people who like the same thing—and that can feed your social rest need too.
But do remember that your social circles – be it a club, a group of friends or a team sport – help to deepen relationships and make you feel more connected. People are dynamic and it’s important to embrace all of your social needs. Whatever you’re into, there is a group of people who like the same thing—and that can feed your social rest need too. You want to think in terms of each of your 5 senses. If you live in a big city, it can be brutally loud, assault you with a myriad of smells from delicious to disgusting, cram you in like sardines during a bus ride, and always have something to look at between the people, cars, buildings, and randomness on every corner. Needless to say, sensory overload can occur!
You want to think in terms of each of your 5 senses. If you live in a big city, it can be brutally loud, assault you with a myriad of smells from delicious to disgusting, cram you in like sardines during a bus ride, and always have something to look at between the people, cars, buildings, and randomness on every corner. Needless to say, sensory overload can occur! If you’ve ever felt like you’re just out of good ideas, you’ve experienced being creatively drained. Most people experience it as being uninspired or feeling blocked from your creative juices. And if you’ve been there, you know that pushing through doesn’t always work.
If you’ve ever felt like you’re just out of good ideas, you’ve experienced being creatively drained. Most people experience it as being uninspired or feeling blocked from your creative juices. And if you’ve been there, you know that pushing through doesn’t always work.
 Mindfulness may indeed have psychological benefits. Earlier this year, a synthesis of randomised controlled trials revealed that mindfulness-based interventions had small to moderate benefits for a number of health outcomes, including stress, anxiety and depression. That said, the effects of mindfulness were smaller and less consistent when compared with those of other therapies, and some effects appeared to fade months after the intervention. Taken together, the results suggest that mindfulness-based interventions may be better than nothing for some outcomes but that more research is needed to compare mindfulness with other therapies.
Mindfulness may indeed have psychological benefits. Earlier this year, a synthesis of randomised controlled trials revealed that mindfulness-based interventions had small to moderate benefits for a number of health outcomes, including stress, anxiety and depression. That said, the effects of mindfulness were smaller and less consistent when compared with those of other therapies, and some effects appeared to fade months after the intervention. Taken together, the results suggest that mindfulness-based interventions may be better than nothing for some outcomes but that more research is needed to compare mindfulness with other therapies. To be clear, paying attention is important when learning a new skill. In a 2019 study, measures of cognitive ability that tapped the capacity to focus attention predicted novice pianists’ ability to learn and play “Happy Birthday to You.”
To be clear, paying attention is important when learning a new skill. In a 2019 study, measures of cognitive ability that tapped the capacity to focus attention predicted novice pianists’ ability to learn and play “Happy Birthday to You.” More recently (2013), psychologist Yannick Balk and his colleagues had golfers try different interventions designed to lessen the effects of performance pressure. The researchers induced performance pressure by videotaping the participants, telling them that their score sheets would be posted publicly at the clubhouse and incentivising strong performance with coupons to the golf shop.
More recently (2013), psychologist Yannick Balk and his colleagues had golfers try different interventions designed to lessen the effects of performance pressure. The researchers induced performance pressure by videotaping the participants, telling them that their score sheets would be posted publicly at the clubhouse and incentivising strong performance with coupons to the golf shop. Nevertheless, the important message from this research is that focusing too carefully on the execution of well-practiced motor sequences can cause mistakes. Of course, we should not resign to go through life on autopilot, missing opportunities to make deeper
Nevertheless, the important message from this research is that focusing too carefully on the execution of well-practiced motor sequences can cause mistakes. Of course, we should not resign to go through life on autopilot, missing opportunities to make deeper
 Hints that grey hairs could spontaneously regain colour have existed as isolated case studies within the scientific literature for decades. In one 1972 paper, the dermatologist Stanley Comaish reported an encounter with a 38-year-old man who had what he described as a “most unusual feature.” Although the vast majority of the individual’s hairs were either all black or all white, three strands were light near the ends but dark near the roots. This signaled a reversal in the normal greying process, which begins at the root.
Hints that grey hairs could spontaneously regain colour have existed as isolated case studies within the scientific literature for decades. In one 1972 paper, the dermatologist Stanley Comaish reported an encounter with a 38-year-old man who had what he described as a “most unusual feature.” Although the vast majority of the individual’s hairs were either all black or all white, three strands were light near the ends but dark near the roots. This signaled a reversal in the normal greying process, which begins at the root. While discussing these ideas with his partner, Picard mentioned something in passing: if one could find a hair that was only partially grey—and then calculate how fast that hair was growing—it might be possible to pinpoint the period in which the hair began aging and thus ask the question of what happened in the individual’s life to trigger this change. He was thinking out loud…but unexpectedly, his wife turned to him and said she had seen such two-coloured hairs on her head. She went to the bathroom, plucked a couple of her own greying hairs—that’s when and how the project started!
While discussing these ideas with his partner, Picard mentioned something in passing: if one could find a hair that was only partially grey—and then calculate how fast that hair was growing—it might be possible to pinpoint the period in which the hair began aging and thus ask the question of what happened in the individual’s life to trigger this change. He was thinking out loud…but unexpectedly, his wife turned to him and said she had seen such two-coloured hairs on her head. She went to the bathroom, plucked a couple of her own greying hairs—that’s when and how the project started! The team also investigated the association between hair greying and psychological stress because prior research hinted that such factors may accelerate the hair’s aging process. Anecdotes of such a connection are also visible throughout history: according to legend, the hair of Marie Antoinette, the 18th-century queen of France, turned white overnight just before her execution at the guillotine.
The team also investigated the association between hair greying and psychological stress because prior research hinted that such factors may accelerate the hair’s aging process. Anecdotes of such a connection are also visible throughout history: according to legend, the hair of Marie Antoinette, the 18th-century queen of France, turned white overnight just before her execution at the guillotine. For now, the next step is to look more carefully at the link between stress and greying. Picard and colleagues are currently putting together a grant to conduct another study that would examine changes in hair and stress levels prospectively—which means tracking participants over a specified period of time rather than asking them to recall life events from the past.
For now, the next step is to look more carefully at the link between stress and greying. Picard and colleagues are currently putting together a grant to conduct another study that would examine changes in hair and stress levels prospectively—which means tracking participants over a specified period of time rather than asking them to recall life events from the past.
 It’s no wonder that nearly 60 percent of psychiatric patients want to discuss spirituality in the context of their treatment. Yet psychiatrists and doctors rarely provide such an opportunity. Since Sigmund Freud’s characterisation of religion as a “mass-delusion” nearly 100 years ago, mental health professionals and scientists have eschewed the spiritual realm. Current efforts to flatten the COVID-19 mental health curve have been almost entirely secular. The American Psychological Association’s extensive set of consumer resources makes no mention of spirituality. And the Centers for Disease Control and Prevention’s only spiritual recommendation is to “connect with your community- or faith-based organisations.” Of more than 90,000 active projects presently funded by all 27 institutes and centers within the National Institutes of Health, fewer than 20 mention spirituality anywhere in the abstract, and only one project contains this term in its title. Needless to say, a lack of funding for research on spirituality hamstrings clinical innovation and dissemination.
It’s no wonder that nearly 60 percent of psychiatric patients want to discuss spirituality in the context of their treatment. Yet psychiatrists and doctors rarely provide such an opportunity. Since Sigmund Freud’s characterisation of religion as a “mass-delusion” nearly 100 years ago, mental health professionals and scientists have eschewed the spiritual realm. Current efforts to flatten the COVID-19 mental health curve have been almost entirely secular. The American Psychological Association’s extensive set of consumer resources makes no mention of spirituality. And the Centers for Disease Control and Prevention’s only spiritual recommendation is to “connect with your community- or faith-based organisations.” Of more than 90,000 active projects presently funded by all 27 institutes and centers within the National Institutes of Health, fewer than 20 mention spirituality anywhere in the abstract, and only one project contains this term in its title. Needless to say, a lack of funding for research on spirituality hamstrings clinical innovation and dissemination.
 Compassion fatigue was first described in emergency department nurses and oncology nurses. Nurses may constantly witness pain, decline, and death, often without being able to save patients no matter how much of themselves they put into their work. Compassion fatigue has also been documented in child protection workers and mental healthcare providers.
Compassion fatigue was first described in emergency department nurses and oncology nurses. Nurses may constantly witness pain, decline, and death, often without being able to save patients no matter how much of themselves they put into their work. Compassion fatigue has also been documented in child protection workers and mental healthcare providers. Having just one or two of these symptoms could be a fluke. But if you’re experiencing a few of these, chances are good that you’re experiencing compassion fatigue.
Having just one or two of these symptoms could be a fluke. But if you’re experiencing a few of these, chances are good that you’re experiencing compassion fatigue. You’ve been giving compassion to your patients or your family or total strangers. But have you been giving any to yourself? Do you forgive yourself for mistakes or cut yourself some slack when you need a break? Do you say to yourself the comforting things that you would say to your best friend? Self-compassion is an important ingredient in loosening up compassion fatigue.
You’ve been giving compassion to your patients or your family or total strangers. But have you been giving any to yourself? Do you forgive yourself for mistakes or cut yourself some slack when you need a break? Do you say to yourself the comforting things that you would say to your best friend? Self-compassion is an important ingredient in loosening up compassion fatigue.

 The research suggests that whatever you think the other person wants, you may well be wrong. The answer seems to be to leave at the first time it seems appropriate, because it’s better to be left wanting more than less.
The research suggests that whatever you think the other person wants, you may well be wrong. The answer seems to be to leave at the first time it seems appropriate, because it’s better to be left wanting more than less. In the second experiment, held in the lab, the researchers split 252 participants into pairs of strangers and instructed them to talk about whatever they liked for anywhere from one to 45 minutes. Afterward the team asked the subjects when they would have liked the conversation to have ended and to guess about their partner’s answer to the same question.
In the second experiment, held in the lab, the researchers split 252 participants into pairs of strangers and instructed them to talk about whatever they liked for anywhere from one to 45 minutes. Afterward the team asked the subjects when they would have liked the conversation to have ended and to guess about their partner’s answer to the same question. That people fail so completely in judging when a conversation partner wishes to wrap things up is quite astounding. Conversations are normally an elegant expression of mutual coordination. And yet it all falls apart at the end because we just can’t figure out when to stop. This puzzle is probably one reason why people like to have talks over coffee, drinks or a meal, because the empty coffee cup or asking for the bill gives us an excuse which is a critical conversation-ending crutch.
That people fail so completely in judging when a conversation partner wishes to wrap things up is quite astounding. Conversations are normally an elegant expression of mutual coordination. And yet it all falls apart at the end because we just can’t figure out when to stop. This puzzle is probably one reason why people like to have talks over coffee, drinks or a meal, because the empty coffee cup or asking for the bill gives us an excuse which is a critical conversation-ending crutch. While this cannot be determined in the countless exchanges of everyday life, scientists could feasibly design an experiment in which talks either end at precisely the point when a participant first wants to stop or continue for some point beyond. Do those whose conversations end just when they want them to actually end up with better conversations than those that last longer?
While this cannot be determined in the countless exchanges of everyday life, scientists could feasibly design an experiment in which talks either end at precisely the point when a participant first wants to stop or continue for some point beyond. Do those whose conversations end just when they want them to actually end up with better conversations than those that last longer? The burgeoning science of conversation obviously needs more rigorous research, but it also needs causal experiments to test strategies that might help us navigate the important and pervasive challenges of conversation. It tickles me that we can put rovers on Mars, have amazing scientific breakthroughs and yet we’re just beginning to rigorously understand how we, as people, talk to each other!!
The burgeoning science of conversation obviously needs more rigorous research, but it also needs causal experiments to test strategies that might help us navigate the important and pervasive challenges of conversation. It tickles me that we can put rovers on Mars, have amazing scientific breakthroughs and yet we’re just beginning to rigorously understand how we, as people, talk to each other!!
 The type of lateralisation most familiar to people is undoubtedly handedness. This has been studied in animals by looking at things like which hand monkeys use to grab something, which paw dogs use to knock food out of a container, and so on. But what do you do when the animal you’re studying doesn’t have hands (or paws)? How do you study lateralisation in an animal like a dolphin?
The type of lateralisation most familiar to people is undoubtedly handedness. This has been studied in animals by looking at things like which hand monkeys use to grab something, which paw dogs use to knock food out of a container, and so on. But what do you do when the animal you’re studying doesn’t have hands (or paws)? How do you study lateralisation in an animal like a dolphin? This is where it gets tricky. When comparing across animals, we have to take account of the fact that body plans and typical ways of moving may be different. For example, if the animal walks upright (like humans and birds) the long axis of its body is vertical, but if it walks on all fours, the long axis of its body is horizontal. This means that “turning” can involve very different types of movements. For an animal on all fours, turning involves crunching the long axis of its body to one side or the other. For an animal on two legs, turning involves spinning around the long axis of its body, which is kept straight. And for an animal like a dolphin who moves in three-dimensional space, either type of turning is possible.
This is where it gets tricky. When comparing across animals, we have to take account of the fact that body plans and typical ways of moving may be different. For example, if the animal walks upright (like humans and birds) the long axis of its body is vertical, but if it walks on all fours, the long axis of its body is horizontal. This means that “turning” can involve very different types of movements. For an animal on all fours, turning involves crunching the long axis of its body to one side or the other. For an animal on two legs, turning involves spinning around the long axis of its body, which is kept straight. And for an animal like a dolphin who moves in three-dimensional space, either type of turning is possible. When scientists set out to study lateralisation in dolphins, they were careful to separate these two different types of turning. But they ran into another problem when researchers kept disagreeing about what counts as a spin “to the right” (or left). After a lot of discussion (and sometimes argument), they realised that they had stumbled upon a weird quirk of human perception. Apparently, humans interpret the direction of spinning in opposite ways depending on the orientation of the animal.
When scientists set out to study lateralisation in dolphins, they were careful to separate these two different types of turning. But they ran into another problem when researchers kept disagreeing about what counts as a spin “to the right” (or left). After a lot of discussion (and sometimes argument), they realised that they had stumbled upon a weird quirk of human perception. Apparently, humans interpret the direction of spinning in opposite ways depending on the orientation of the animal. The system they came up with was actually inspired by the “right-hand rule” of electromagnetism that many of us learned in school physics lessons. According to that rule, if you point your right thumb in the direction in which an electrical current flows through a wire, the curve of your fingers shows you the direction of the magnetic field flowing around that wire. The dolpihn researchers adopted the general outline of this schematic model to create the Right-Fingered Spin (RiFS) versus Left-Fingered Spin (LeFS) coding system. In this system, when a coder’s outstretched thumb is oriented along the animal’s long axis, pointed toward its head, the curled fingers of the relevant hand describe the direction of rotation. This allowed us to quickly and unambiguously code spinning/turning behaviours no matter the animal’s orientation or direction of movement.
The system they came up with was actually inspired by the “right-hand rule” of electromagnetism that many of us learned in school physics lessons. According to that rule, if you point your right thumb in the direction in which an electrical current flows through a wire, the curve of your fingers shows you the direction of the magnetic field flowing around that wire. The dolpihn researchers adopted the general outline of this schematic model to create the Right-Fingered Spin (RiFS) versus Left-Fingered Spin (LeFS) coding system. In this system, when a coder’s outstretched thumb is oriented along the animal’s long axis, pointed toward its head, the curled fingers of the relevant hand describe the direction of rotation. This allowed us to quickly and unambiguously code spinning/turning behaviours no matter the animal’s orientation or direction of movement. People often think that scientific progress happens when we learn something new that we didn’t know before. But another kind of scientific progress happens when we realise that there is a problem with the way we’ve been looking at things all along. In those cases, figuring out a different way of looking can lead to seeing things more clearly. And as science fiction writer Isaac Asimov once pointed out, “The most exciting phrase to hear in science, the one that heralds new discoveries, is not “Eureka!’ but ‘That’s funny…’”
People often think that scientific progress happens when we learn something new that we didn’t know before. But another kind of scientific progress happens when we realise that there is a problem with the way we’ve been looking at things all along. In those cases, figuring out a different way of looking can lead to seeing things more clearly. And as science fiction writer Isaac Asimov once pointed out, “The most exciting phrase to hear in science, the one that heralds new discoveries, is not “Eureka!’ but ‘That’s funny…’”
 The Danish believe in hygge (pronounced “hoo-gah”), which loosely translates to “coziness” and sounds to me a lot like ‘hug’! The word originated from an Old Norwegian word meaning “well-being,” and it captures all that is cozy, warm, and enjoyable. Curling up under a soft blanket while holding a warm mug of cocoa is hygge. Chatting with friends and family around a fire (ohhh I wish that that were possible at the moment….) is hygge. And simply enjoying the glow of a candle is hygge.
The Danish believe in hygge (pronounced “hoo-gah”), which loosely translates to “coziness” and sounds to me a lot like ‘hug’! The word originated from an Old Norwegian word meaning “well-being,” and it captures all that is cozy, warm, and enjoyable. Curling up under a soft blanket while holding a warm mug of cocoa is hygge. Chatting with friends and family around a fire (ohhh I wish that that were possible at the moment….) is hygge. And simply enjoying the glow of a candle is hygge. On the subject of being with the environment, we’ll ‘travel’ now eastwards to Japan, to take a dip in the woods. Not an actual swim, but rather, an immersion in nature called “shinrin-yoku,” loosely translated to “forest bathing.”
On the subject of being with the environment, we’ll ‘travel’ now eastwards to Japan, to take a dip in the woods. Not an actual swim, but rather, an immersion in nature called “shinrin-yoku,” loosely translated to “forest bathing.” Who doesn’t enjoy a good belly laugh? But have you ever done it on purpose? The idea of (Indian) laughter yoga is that we don’t have to wait for something funny to happen in order to laugh. Instead, laughter can and should be practiced for its own sake.
Who doesn’t enjoy a good belly laugh? But have you ever done it on purpose? The idea of (Indian) laughter yoga is that we don’t have to wait for something funny to happen in order to laugh. Instead, laughter can and should be practiced for its own sake.
 Dopamine production is essential for growth. But there are so many misconceptions about the role of dopamine in cognition and behaviour. Dopamine is often labelled the “feel-good molecule,” but this is a gross mischaracterisation of this neurotransmitter. As personality neuroscientist Colin DeYoung notes, dopamine is actually the “neuromodulator of exploration.” Dopamine’s primary role is to make us want things, but not necessarily like things. We get the biggest rush of dopamine coursing through our brains at the possibility of reward, but this rush is no guarantee that we’ll actually like or even enjoy the thing once we get it. Dopamine is a huge energising force in our lives, driving our motivation to explore and facilitating the cognitive and behavioural processes that allow us to extract the most delights from the unknown.
Dopamine production is essential for growth. But there are so many misconceptions about the role of dopamine in cognition and behaviour. Dopamine is often labelled the “feel-good molecule,” but this is a gross mischaracterisation of this neurotransmitter. As personality neuroscientist Colin DeYoung notes, dopamine is actually the “neuromodulator of exploration.” Dopamine’s primary role is to make us want things, but not necessarily like things. We get the biggest rush of dopamine coursing through our brains at the possibility of reward, but this rush is no guarantee that we’ll actually like or even enjoy the thing once we get it. Dopamine is a huge energising force in our lives, driving our motivation to explore and facilitating the cognitive and behavioural processes that allow us to extract the most delights from the unknown. How active is your nerdy dopamine pathway?
How active is your nerdy dopamine pathway?
 But what kind of phenomenon is this, exactly? Why was it happening with such vigour? To find out, Deirdre Barrett, an assistant professor at Harvard University and editor in chief of the journal Dreaming, initiated a COVID-19 dreams survey online in the week of March 22. Erin and Grace Gravley, San Francisco Bay Area artists, launched IDreamofCovid.com, a site archiving and illustrating pandemic dreams. The Twitter account @CovidDreams began operation. Kelly Bulkeley, a psychologist of religion and director of the Sleep and Dream Database, followed with a YouGov survey of 2,477 American adults. Postdoctoral research fellow Elizaveta Solomonova, at McGill University, along with Rebecca Robillard of the Royal’s Institute of Mental Health Research in Ottawa and others, launched a survey to which 968 people aged 12 and older responded, almost all in North America. Results of these inquiries, not yet published in journals but available in preliminary form online, document the precipitous surge, the striking variety of dreams and many related mental health effects.
But what kind of phenomenon is this, exactly? Why was it happening with such vigour? To find out, Deirdre Barrett, an assistant professor at Harvard University and editor in chief of the journal Dreaming, initiated a COVID-19 dreams survey online in the week of March 22. Erin and Grace Gravley, San Francisco Bay Area artists, launched IDreamofCovid.com, a site archiving and illustrating pandemic dreams. The Twitter account @CovidDreams began operation. Kelly Bulkeley, a psychologist of religion and director of the Sleep and Dream Database, followed with a YouGov survey of 2,477 American adults. Postdoctoral research fellow Elizaveta Solomonova, at McGill University, along with Rebecca Robillard of the Royal’s Institute of Mental Health Research in Ottawa and others, launched a survey to which 968 people aged 12 and older responded, almost all in North America. Results of these inquiries, not yet published in journals but available in preliminary form online, document the precipitous surge, the striking variety of dreams and many related mental health effects. More recent studies found qualitative changes in dream emotions and concerns about health. Dream reports from Brazilian adults in social isolation had high proportions of words related to anger, sadness, contamination and cleanliness. Text mining of accounts of 810 Finnish dreams showed that most word clusters were laden with anxiousness; 55 percent were about the pandemic directly (lack of regard for social distancing, elderly people in trouble), and these emotions were more prevalent among people who felt increased stress during the day. A study of 100 nurses conscripted to treat COVID-19 patients in Wuhan, China, revealed that 45 percent experienced nightmares—twice the lifetime rate among Chinese psychiatric outpatients and many times higher than that among the 5 percent of the general population who have nightmare disorder.
More recent studies found qualitative changes in dream emotions and concerns about health. Dream reports from Brazilian adults in social isolation had high proportions of words related to anger, sadness, contamination and cleanliness. Text mining of accounts of 810 Finnish dreams showed that most word clusters were laden with anxiousness; 55 percent were about the pandemic directly (lack of regard for social distancing, elderly people in trouble), and these emotions were more prevalent among people who felt increased stress during the day. A study of 100 nurses conscripted to treat COVID-19 patients in Wuhan, China, revealed that 45 percent experienced nightmares—twice the lifetime rate among Chinese psychiatric outpatients and many times higher than that among the 5 percent of the general population who have nightmare disorder. Longer slumber leads to more dreams; people in sleep laboratories who are allowed to snooze more than 9.5 hours recall more dreams than when sleeping a typical eight hours. Sleeping longer also proportionally increases rapid eye movement (REM) sleep, which is when the most vivid and emotional dreams occur.
Longer slumber leads to more dreams; people in sleep laboratories who are allowed to snooze more than 9.5 hours recall more dreams than when sleeping a typical eight hours. Sleeping longer also proportionally increases rapid eye movement (REM) sleep, which is when the most vivid and emotional dreams occur. One way to understand direct and metaphoric imagery is to consider that dreams express an individual’s core concerns, drawing on memories that are similar in emotional tone but different in subject matter. This contextualisation is clear in post-traumatic nightmares, in which a person’s reaction to a trauma, such as terror during an assault, is depicted as terror in the face of a natural disaster such as a tsunami. The late Ernest Hartmann, a Boston-area dream and nightmare research pioneer who studied dreams after the 9/11 attacks, stipulated that such contextualisation best helps people adapt when it weaves together old and new experiences. Successful integration produces a more stable memory system that is resilient to future traumas.
One way to understand direct and metaphoric imagery is to consider that dreams express an individual’s core concerns, drawing on memories that are similar in emotional tone but different in subject matter. This contextualisation is clear in post-traumatic nightmares, in which a person’s reaction to a trauma, such as terror during an assault, is depicted as terror in the face of a natural disaster such as a tsunami. The late Ernest Hartmann, a Boston-area dream and nightmare research pioneer who studied dreams after the 9/11 attacks, stipulated that such contextualisation best helps people adapt when it weaves together old and new experiences. Successful integration produces a more stable memory system that is resilient to future traumas. Other investigators, such as cognitive neuroscientist Antti Revonsuo of the University of Turku in Finland, have since proposed additional social functions for dreaming: facilitating social perception (who is around me?), social mind reading (what are they thinking?) and the practice of social bonding skills. Another theory advanced by psychology professor Mark Blagrove of Swansea University in Wales further postulates that by sharing dreams, people enhance empathy toward others. The range of dream functions is likely to keep expanding as we learn more about the brain circuits underlying social cognition and the roles REM sleep plays in memory for emotional stimuli, human faces and reactions to social exclusion. Because social distancing is, in effect, an experiment in social isolation at a level never before seen—and is likely antagonistic to human evolution—a clash with deep-rooted dream mechanisms should be evident on a massive scale. And because social distancing disrupts normal relationships so profoundly—causing many of us to spend excessive time with some people and no time with others—social simulations in dreams may play a crucial role in helping families, groups, even societies deal with sudden, widespread social adaptation.
Other investigators, such as cognitive neuroscientist Antti Revonsuo of the University of Turku in Finland, have since proposed additional social functions for dreaming: facilitating social perception (who is around me?), social mind reading (what are they thinking?) and the practice of social bonding skills. Another theory advanced by psychology professor Mark Blagrove of Swansea University in Wales further postulates that by sharing dreams, people enhance empathy toward others. The range of dream functions is likely to keep expanding as we learn more about the brain circuits underlying social cognition and the roles REM sleep plays in memory for emotional stimuli, human faces and reactions to social exclusion. Because social distancing is, in effect, an experiment in social isolation at a level never before seen—and is likely antagonistic to human evolution—a clash with deep-rooted dream mechanisms should be evident on a massive scale. And because social distancing disrupts normal relationships so profoundly—causing many of us to spend excessive time with some people and no time with others—social simulations in dreams may play a crucial role in helping families, groups, even societies deal with sudden, widespread social adaptation. Once stories emerged, additional surges in dream reporting through early April were detected by @CovidDreams and IDreamofCovid.com. The format of most early stories almost guaranteed amplification: they typically described some salient dream themes observed in a survey and provided a link directing readers to participate in the same survey. In addition, 56 percent of articles during the first week of stories featured interviews with the same Harvard dream scientist, which may have influenced readers to dream about the themes repeated by her in various interviews.
Once stories emerged, additional surges in dream reporting through early April were detected by @CovidDreams and IDreamofCovid.com. The format of most early stories almost guaranteed amplification: they typically described some salient dream themes observed in a survey and provided a link directing readers to participate in the same survey. In addition, 56 percent of articles during the first week of stories featured interviews with the same Harvard dream scientist, which may have influenced readers to dream about the themes repeated by her in various interviews.
 In the study, researchers at Wageningen University & Research in the Netherlands observed 512 participants follow a fixed path through a room where either eight food samples or eight food-scented cotton pads were placed in different locations. When they arrived at a sample, the participants would taste the food or smell the cotton and rate how much they liked it. Four of the food samples were high-calorie, including brownies and potato chips, and the other four, including cherry tomatoes and apples, were low in calories—’diet foods’, you might call them.
In the study, researchers at Wageningen University & Research in the Netherlands observed 512 participants follow a fixed path through a room where either eight food samples or eight food-scented cotton pads were placed in different locations. When they arrived at a sample, the participants would taste the food or smell the cotton and rate how much they liked it. Four of the food samples were high-calorie, including brownies and potato chips, and the other four, including cherry tomatoes and apples, were low in calories—’diet foods’, you might call them. We tend to think of primates such as ourselves as having lost the acute sense of smell seen in many other mammals in favour of sharp eyesight. And to a large degree, we humans have developed that way. But the new findings support the notion that our sniffer is not altogether terrible: These results suggest that human minds continue to house a system optimised for ‘energy‐efficient foraging’ within erratic food habitats of the past. And it highlights the often underestimated capabilities of the human sense of smell.
We tend to think of primates such as ourselves as having lost the acute sense of smell seen in many other mammals in favour of sharp eyesight. And to a large degree, we humans have developed that way. But the new findings support the notion that our sniffer is not altogether terrible: These results suggest that human minds continue to house a system optimised for ‘energy‐efficient foraging’ within erratic food habitats of the past. And it highlights the often underestimated capabilities of the human sense of smell.