DOWNLOAD THE ENTIRE JANUARY 2017 NEWSLETTER including this month’s Freebie.
The fact that exercise improves physical health is so well known as to be a platitude. Decades of research demonstrate that regular exercise lowers the risk of many illnesses—heart disease, obesity, diabetes, cancer—and extends the average life span. In contrast, the benefits of exercise for mental health are not quite so obvious or well publicised. We work out to “get in shape,” and some of us depend on bike rides, neighbourhood jogs or yoga to help clear our mind and relieve stress. But how often do we seriously consider exercise as a viable treatment for mental illness, one just as effective as medication or counselling? Can a steady routine of physical workouts really help to keep psychological disorders in check?
In the case of depression, the collective evidence to date suggests that the answer is an emphatic yes. Exercise is by no means a panacea, and in severe cases of depression, it may be futile on its own. But scores of experiments now show that exercise is much more than a temporary distraction from mental woes or some ultimately inconsequential palliative. It appears to combat depression in a number of ways: by strengthening our biochemical resilience to stress, encouraging the growth of new brain cells, bolstering self-esteem and possibly even counterbalancing an underlying genetic risk for mental illness. For most people with mild to moderate depression, exercise is one of the strongest, safest, most practical, most affordable and even enjoyable treatments available.
On the Strength of the Evidence
Major depression— an illness characterised by a persistent low mood or loss of interest in typically pleasurable activities, often accompanied by insomnia, fatigue, poor concentration or feelings of worthlessness—is one of the  leading causes of disability and death around the globe, according to the World Health Organisation. At any given time, it afflicts around 350 million people worldwide. Only a fraction of sufferers seek help, and of those, only a third respond to standard treatment, which is usually counselling and medication. Antidepressant drugs are often costly and can have serious side effects, driving many patients to search for less expensive, safer, more natural solutions. In a survey of more than 2,000 U.S. adults published in 2001, more than half of the respondents with depression said that they had turned to some kind of alternative treatment, such as yoga, herbal medicines or acupuncture.
leading causes of disability and death around the globe, according to the World Health Organisation. At any given time, it afflicts around 350 million people worldwide. Only a fraction of sufferers seek help, and of those, only a third respond to standard treatment, which is usually counselling and medication. Antidepressant drugs are often costly and can have serious side effects, driving many patients to search for less expensive, safer, more natural solutions. In a survey of more than 2,000 U.S. adults published in 2001, more than half of the respondents with depression said that they had turned to some kind of alternative treatment, such as yoga, herbal medicines or acupuncture.
Psychologists and clinicians have studied exercise as an alternative treatment for depression for at least 30 years. James Blumenthal at Duke University in the U.S. was one of the pioneers. In the 1980s, while researching how exercise helps patients with cardiovascular disease, he and his colleagues noticed an inadvertent secondary benefit: working out seemed to improve people’s moods and reduce symptoms of depression. They decided to investigate. One of their early studies, published in 1999, tracked the health of 156 elderly men and women diagnosed with depression as they exercised regularly or took antidepressants, or both. After 16 weeks, all three groups had improved equally, but relapse rates were lowest among patients who exercised.
In a follow-up study, published a decade later, they divided more than 200 adults with depression into four groups, each receiving a different intervention: supervised exercise classes, exercise at home, medication or placebo. They found that patients engaging in supervised exercise fared better than those working out at home and achieved nearly equivalent remission rates as those taking antidepressants: 45 versus 47 percent, respectively. By comparison, the home exercise group reached a 40 percent remission rate and the placebo group, 31 percent.
More recently, in a similar study in 2015, Swedish scientists assigned 946 patients with mild to moderate depression to one of three 12-week treatments: three-times-a-week sessions of yoga, aerobics or strength training; Internet-based cognitive-behavioural therapy; or standard counselling plus medication. Patients in all groups improved, but those engaging in exercise experienced the greatest benefits. Internet-based therapy came in as a close runner-up, but the typical standard treatment plan lagged behind both alternatives.
To date, numerous meta-analyses have kept score on the accumulating data. They do not all agree: a few have found no indication that exercise is helpful or have found that it offers only very small effects or greatly diminished benefits in the long term. But most have reached similar optimistic conclusions. A 2013 review by the nonprofit organization Cochrane, regarded as a leader in evidence- based medicine, concluded that exercise is just as effective a treatment for depression as medication and counseling.
A recent meta-analysis, published in 2016, echoes Cochrane’s finding. A team of international researchers examined 25 of the most rigorous experiments and determined that exercise, especially moderate to vigorous aerobic exercise under professional supervision, is indeed a potent treatment for depression. When they adjusted their analysis to account for ‘weak studies’—those most prone to some kind of experimental bias—they found an even stronger effect, suggesting that some previous meta-analyses may have underestimated exercise’s benefits for mental health. The researchers further calculated that it would take at least 1,000 contradictory studies to negate the affirming evidence that has piled up so far. Yet another review computed that when exercise is used to treat depression, success rates increase by as much as 67 to 74 percent.
How Much Is Enough?
 Some researchers have attempted to figure out what types of exercise and intensity levels are most effective as an anti-depressant. In a frequently cited study from 2005, for example, psychiatrist Madhukar Trivedi (University of Texas Southwestern Medical Center) and his colleagues tracked the health of 80 adults with mild to moderate depression for three months as they exercised three to five times a week on a treadmill or stationary bicycle at low intensity (seven kilocalories per kilogram per week) or at a higher intensity, as recommended by public health authorities (17.5 kilocalories per kilogram per week). At the end of the three months, the adults who exercised at the higher intensity had lessened the severity of their depression by 47 percent, compared with only 30 percent for the low-intensity group and 29 percent for a group who engaged in stretching rather than aerobic exercise.
Some researchers have attempted to figure out what types of exercise and intensity levels are most effective as an anti-depressant. In a frequently cited study from 2005, for example, psychiatrist Madhukar Trivedi (University of Texas Southwestern Medical Center) and his colleagues tracked the health of 80 adults with mild to moderate depression for three months as they exercised three to five times a week on a treadmill or stationary bicycle at low intensity (seven kilocalories per kilogram per week) or at a higher intensity, as recommended by public health authorities (17.5 kilocalories per kilogram per week). At the end of the three months, the adults who exercised at the higher intensity had lessened the severity of their depression by 47 percent, compared with only 30 percent for the low-intensity group and 29 percent for a group who engaged in stretching rather than aerobic exercise.
On the basis of studies such as this one, some psychologists, clinicians and health authorities have gone as far as publishing specific recommendations. Trivedi prescribes three to five 45- to 60-minute sessions of aerobic exercise (walking, running, cycling, or using a treadmill, stationary bike or elliptical trainer) each week at an intensity of 50 to 85 percent maximum heart rate. “The ideal is probably at least 16 kilocalories per kilogram of body weight, which works out to 1,200 to 1,500 kilocalories each week for average body weight,” Trivedi says. “If you can talk to your spouse on the phone, you’re not working out at the right intensity.”
Likewise Central Queensland University exercise psychologist Robert Stanton advises 30- to 40-minute sessions of aerobic exercise—walking, cross training or stationary cycling—three to four times a week at low to moderate intensity for at least nine weeks. And the National Institute for Health and Care Excellence advocates group-based physical activity programs for patients with mild to moderate depression, consisting of at least three 45-minute sessions a week for at least 10 weeks.
Other experts, however, think it may be too soon to get so specific. A 2013 reiew paper, for instance, concluded that both cardiovascular and resistance exercise, either alone or in combination, are effective at treating depression but that there are not yet enough data to definitively favour one form of physical activity over another.
Why Exercise Works
In the past decade scientists have uncovered numerous details about how exercise alters the brain, and the body as a whole, in ways that alleviate and protect against depression. The second you start running, pedaling or lifting a dumbbell, your body’s chemistry begins to change. Exercise boosts your heart rate, sending blood, oxygen, hormones and neuro-chemicals surging through the body. In the moment, the body responds to exercise as a kind of stress—but it is ultimately beneficial. Some evidence suggests that habitual moderate exercise rewires the brain and immune system to better cope with physical and mental strain. The better the body becomes at dealing with stressors of all kinds, the lower the risk of a depressive episode. In fact, many researchers think of depression as a disorder of managing stress.
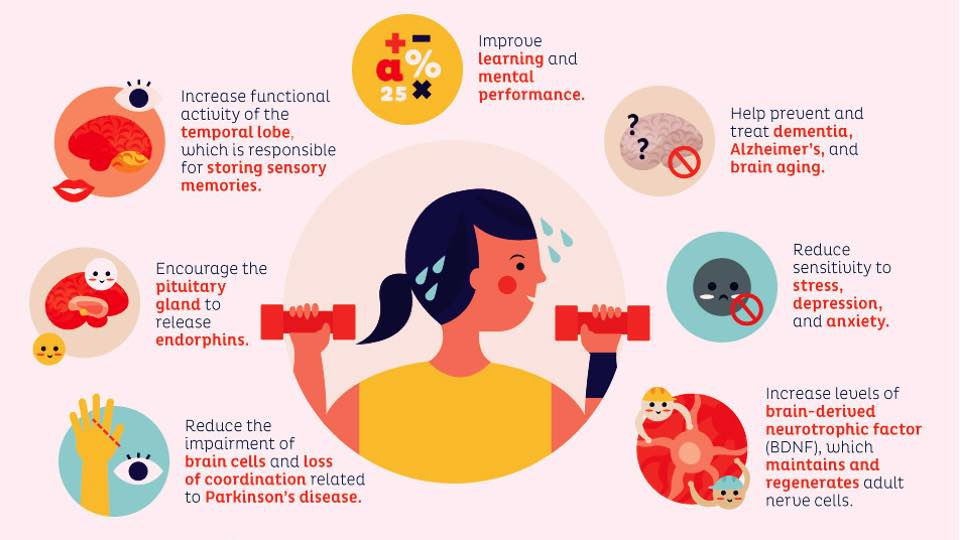 Exercise also seems to mimic some of the chemical effects of antidepressant medication. Based on increasing evidence, some scientists argue that certain cases of depression result from the impaired growth of both brain cells and the connections between them. Studies have documented the atrophy and loss of neurons in brain regions such as the amygdala, hippocampus and prefrontal cortex in patients with major depression. Antidepressants that increase levels of serotonin and other neurotransmitters might work by reinvigorating neural proliferation, a process that depends in part on a molecule called brain-derived neurotrophic factor (BDNF). In studies with both animals and people, exercise enhances the production of BDNF.
Exercise also seems to mimic some of the chemical effects of antidepressant medication. Based on increasing evidence, some scientists argue that certain cases of depression result from the impaired growth of both brain cells and the connections between them. Studies have documented the atrophy and loss of neurons in brain regions such as the amygdala, hippocampus and prefrontal cortex in patients with major depression. Antidepressants that increase levels of serotonin and other neurotransmitters might work by reinvigorating neural proliferation, a process that depends in part on a molecule called brain-derived neurotrophic factor (BDNF). In studies with both animals and people, exercise enhances the production of BDNF.
In one 2001 study, for example, rats given an antidepressant and the opportunity to run produced higher levels of BDNF compared with animals that only ran or only received medication. Moreover, they were better at enduring a stressful experience, swimming for longer in an inescapable water tank before giving up—a test designed to approximate the onset of depression. In an analogous human study in 2016, Brazilian researchers divided 57 adults taking the antidepressant sertraline for moderate to severe depression into two groups: one attended four weekly sessions of aerobic activity for 28 days, and the other did not exercise. Symptoms abated similarly in both groups, but the exercise group improved on lower doses of antidepressants. The authors suspect that exercise enhanced the biochemical effects of the drugs. Similar studies have shown that simply recommending healthy lifestyle changes, such as establishing better sleep routines and getting more exercise, can dramatically boost the efficacy of antidepressants from a mere 10 percent remission rate with the drugs alone to a 60 percent remission rate.
And in a small but intriguing 2015 study, physician Helmuth Haslacher and his colleagues at the Medical University of Vienna compared the mental health and genomes of 55 elderly marathon runners and endurance bicyclists with those of 58 nonathletes. Among the nonathletes, they found a statistically significant correlation between the number of depressive symptoms these individuals experienced and a particular gene variant that interferes with normal BDNF production. Among the athletes, however, there was no such correlation. The researchers concluded that by stimulating BDNF production, long-term, vigorous aerobic exercise might actually counteract a genetic susceptibility to depression.
Neurobiology may also explain why, in addition to exercise countering depression, the inverse seems to be true: correlations in epidemiological surveys suggest that physical inactivity, while sometimes the result of depression, may also be a major risk factor for subsequently developing it. In a 2014 study of more than 6,000 elderly U.K. citizens, the more time they spent watching television, the more likely they were to report symptoms of depression (although this was not true for other sedentary activities such as reading). Those who participated in some form of vigorous physical activity at least once a week experienced less depression. Likewise, a 2015 survey of nearly 5,000 Chinese college students found that the more time a student spent in front of a TV or computer screen, the more likely he or she was to have depressive symptoms. In contrast, the risk for depression dropped the more physically active a student was, regardless of age, gender or residential background. A meta-analysis of 24 studies, involving nearly 200,000 participants, reached the same conclusion: sedentary behaviour was associated with an increased risk of depression. On average, active people are 45 percent less likely to be depressed than inactive people, according to the U.S. Office of Disease Prevention and Health Promotion.
The Feel-Good Factor
Beyond these physiological reasons, many social and psychological factors help to explain why working out can alleviate symptoms of depression. In comprehensive interviews, people who have struggled with the disorder say that exercise energises them, gives them a sense of purpose and achievement, elevates their self-esteem and mood, regulates appetite and sleep cycles, and distracts them from negative thoughts. For those who exercise in a group, it can also provide a welcome opportunity for social interaction.
First, though, many people with depression must overcome a severe lack of motivation. Jennifer Carter, director of sport psychology at the Ohio State University Wexner Medical Center, has come up with a bevy of practical tips, for example, “There are 1,440 minutes in a day. Perhaps you can find 30 of those to exercise.” Getting over that initial hurdle of low motivation seems to depend in particular on how much satisfaction and self-agency people experience while working out. Enjoyment is fundamentally linked to how much people stick with exercise. If you do what is most fun and entertaining, whatever that might be, then you are more likely to stick to it. Research suggests that exercise as therapy succeeds when people choose the type and intensity. Most people prefer a moderate intensity, around or just below the ventilatory threshold—the point at which breathing becomes noticeably laboured. In 2011 Patrick Callaghan, head of health sciences at the University of Nottingham in England, and his colleagues asked 38 women with depression to exercise on treadmills in small groups three times a week, either at a prescribed intensity or one they personally selected. After a month, the women who chose how much to exert themselves had lower levels of depression and higher self-esteem compared with the other group.
 Despite the mounting evidence that exercise can remedy some forms of depression, skepticism persists in academia and health care. Trivedi has found that there is a general bias that exercise is not a bona fide treatment—it’s just something you should do in addition to treatment, like trying to sleep and eat well. Even though recognition of exercise as a treatment is increasing, only some health insurance companies pay for gym time, and when they do, they often offer small temporary discounts.
Despite the mounting evidence that exercise can remedy some forms of depression, skepticism persists in academia and health care. Trivedi has found that there is a general bias that exercise is not a bona fide treatment—it’s just something you should do in addition to treatment, like trying to sleep and eat well. Even though recognition of exercise as a treatment is increasing, only some health insurance companies pay for gym time, and when they do, they often offer small temporary discounts.
Patients will need to change their thinking as well. It can be hard for patients to think of exercise as a form of treatment, since we usually exercise to look good and/or to lose weight. Most individuals do not understand the degree to which exercise can reshape their mood, too. Even if you feel like falling apart and doing nothing, exercise will get you out and about. Depression makes you feel like everything you are about to do is useless and pointless – and that is exactly what exercise fights: you have to get up and go!
REFERENCES
■ Exercise for Depression. G. M. Cooney et al. in Cochrane Database of Systematic Reviews, No. 9, Article No. CD004366; 2013.
■ Physical Exercise Counteracts Genetic Susceptibility to Depression. H. Haslacher et al. in Neuropsychobiology, Vol. 71, No. 3, pages 168–175; May 2015.
■ Exercise as a Treatment for Depression: A Meta-analysis Adjusting for Publication Bias. Felipe b. Schuch et al. in Journal of Psychiatric Research, Vol. 77, pages 42–51; June 2016.
From Our Archives
■ The New Group Therapy. Tegan Cruwys, S. Alexander Haslam and Genevieve A. Dingle; September/October 2014.
■ Head Strong. Ferris Jabr in Scientific American Mind, volume 28, number 1, pages 26-31; January/February 2017.